AI-Smart Custom Ambulatory Software Development: What to Build, What to Buy, and How to Extend

Slava Khristich



Vlad Nazarov

If you run an outpatient practice or health system service line, this article gives you a practical map for custom ambulatory software development—from healthcare system architecture and integration patterns to where custom AI agent development belongs.
You’ll learn how to evaluate build vs. buy, how to extend existing software with agents and automations, and which metrics matter when you deploy. The goal: faster access, fewer bottlenecks, clearer financials for medical organizations.
First, a quick grounding. In U.S. health policy, “ambulatory” generally means care delivered on an outpatient basis without an inpatient admission. A formal legal anchor appears in Medicare rules for Ambulatory Surgical Centers (ASCs), defined as entities operating exclusively to furnish surgical services to patients not requiring hospitalization, with an expected duration under 24 hours (42 CFR 416.2).
| If you require immediate help with custom ambulatory software development solutions, feel free to contact our support team today → |
Ambulatory care is not a niche: Americans make about 1.0 billion physician-office visits each year; hospital outpatient and ambulatory sites absorb a vast share of diagnostics, procedures, and follow-ups. Meanwhile, the number of Medicare-certified ASCs reached ~6,308 in 2023, reflecting a continued site-of-care shift from inpatient to outpatient. Hospital spending represented about 31% of total U.S. health expenditures in 2023, so efficiency in ambulatory workflows has a system-level impact.
Below, we translate that context into custom healthcare software development decisions: which capabilities to implement first, where AI agents provide real lift, and how to connect your stack safely to clinical, revenue, and patient-facing systems.
Why TATEEDA is qualified to talk about ambulatory system development
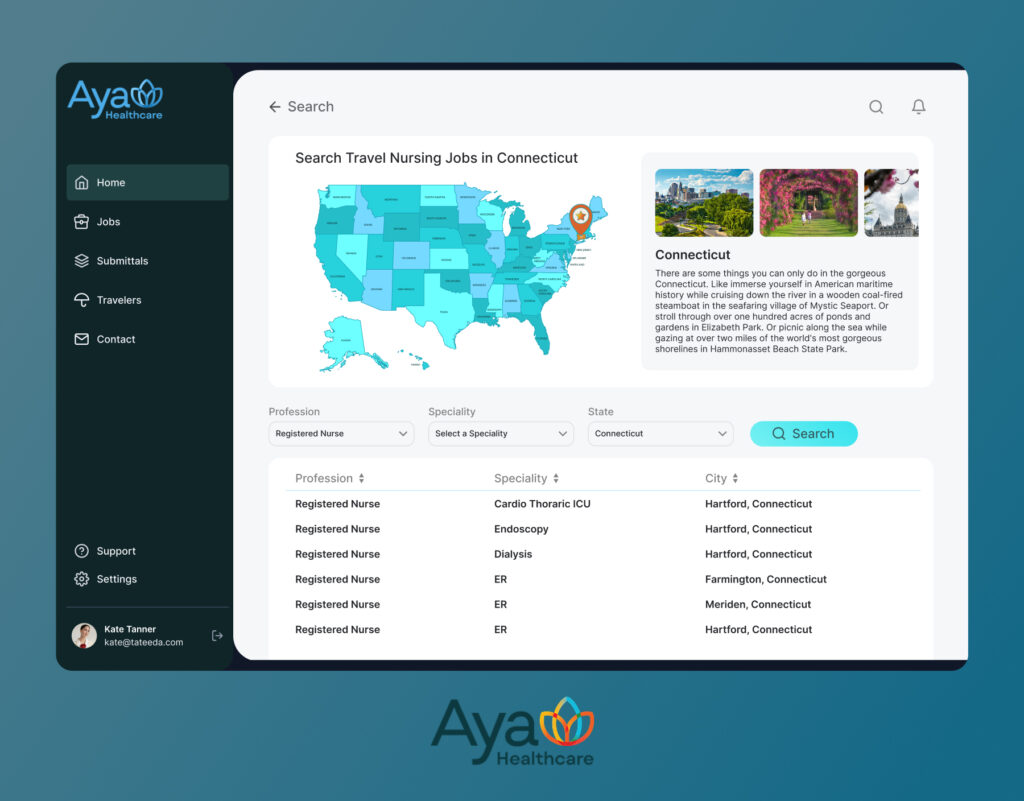
We have shipped production-grade ambulatory platforms at scale. For AYA Healthcare, one of the nation’s largest clinician staffing organizations in the U.S.A., our team delivered custom patient & clinician portals, mobile apps, referral and scheduling flows, and revenue operations.
The stack reflects outpatient reality: FHIR R4 resources for patient, coverage, appointment, and claim; HL7 v2 interfaces for ADT, ORM, and ORU; X12 pipelines for 270/271 eligibility, 276/277 status, 837 submission, and 835 remittance. Identity is handled with enterprise SSO and OAuth 2.0, with PKCE on mobile. Every action lands in an immutable audit trail that meets HIPAA expectations.
Beyond that flagship build, we deliver custom ambulatory software development services with…
- secure two-way messaging
- rules-aware self-scheduling with waitlists
- AI-assisted intake and document capture
- price transparency, plus payment plans.
Our custom medical billing software development services raise first-pass accuracy and speed reimbursement via edits, authorization checks, and clean remittance posting.
With versioned models and human review for low-confidence cases, outpatient teams move faster, patients get clearer touchpoints, and financials stabilize without compromising compliance.
Learn more: ➡️ How to Integrate Optum APIs into Custom Healthcare Software
Table of Contents
How Custom Ambulatory Software Helps Outpatient Operations
Ambulatory organizations cope with high visit volume, tight margins, and a maze of payer rules. Purpose-built software reduces manual handoffs, exposes actionable data at the right moment, and protects staff time. Here’s how custom ambulatory software development services typically translate into day-to-day gains:
- Identity, access, and consent orchestration: Unify patient and caregiver identities across portal, mobile, and telehealth; support proxies; capture consent snapshots with timestamps; enforce SSO and step-up authentication for sensitive flows. AI agents can pre-classify requests (clinical vs. admin) based on message content before routing.
- Eligibility and benefits at scheduling: Embed instant eligibility queries before slot selection; present out-of-pocket ranges in clear language; flag referral/prior-auth prerequisites. An AI rules aide explains benefit caveats in plain English and suggests lower-cost sites when appropriate.
- Configurable scheduling with waitlists: Build templates for procedure blocks, resource pools, and location rules; auto-release no-show risk slots to waitlisted patients. Agents watch for churn signals and push reschedule links when transportation or childcare issues appear in messages.
- Digital intake and e-forms: Replace clipboards with adaptive forms that change by visit type; capture IDs/insurance cards via camera; reconcile meds/allergies with the chart. An AI document reader extracts structured fields from uploads and flags inconsistencies for staff review.
- Two-way messaging and triage: Separate clinical from administrative threads; route by specialty, location, and urgency; apply SLAs. Language detection and summarization help staff scan complex threads quickly; sensitive content triggers escalation policies.
- Telehealth and RPM hooks: One-click video visits with device pre-checks; remote readings (e.g., BP, glucose) flow into clinician queues with thresholds; AI surfaces trends and outliers rather than raw streams.
- Education and adherence tracks: Post-visit micro-lessons and reminders tuned to procedure type, comprehension checks, and adherence signals appearing on care-team dashboards. Agents rephrase instructions at a sixth-grade reading level on request.
- Payments and plans: Itemized statements, payment-plan builders, card-on-file tokens, and gentle nudges tied to payroll cycles. An AI helper explains EOBs, answers “why is this balance different?” and reduces billing calls.
- Operational analytics: Dashboards for show rates, message closure times, auth turnaround, and payment conversion; drill-downs by site, provider, payer. Agents draft weekly highlights—“what moved and why”—for managers.
This is where custom ambulatory software development solutions earn their keep: integrations and decisioning tuned to your specialties, sites, and payer mix, not generic workflows.

Learn more: ➡️ How athenahealth EHR Integration Transforms Patient Data Workflows
A Quick Look at Off-the-Shelf Ambulatory Products
Commercial platforms cover much of the ground, but each has trade-offs you should plan around if you adopt or extend them.
- Epic (EpicCare Ambulatory and related modules)
Comprehensive outpatient workflows with deep integration across registration, orders, documentation, and billing; powerful but complex and resource-intensive to govern. Community-hosted options like OCHIN Epic provide managed footprints for clinics. Expect strength in enterprise cohesion, with customization gated by governance and upgrade cycles. - Oracle Health (Cerner) Ambulatory EHR
Cloud-enabled ambulatory suite emphasizing workflow streamlining, interoperability, and analytics; Oracle highlights ASC and ambulatory solutions with integration and scalability claims. Solid connectivity, though multi-product footprints may require careful interface management and data mapping. - athenaOne (athenahealth)
Cloud EHR/PM with embedded automation and growing AI assistants across medical documentation, scheduling, and communications; strengths include managed services and connectivity, while trade-offs can include reliance on vendor-managed processes and standardized templates that may limit niche customization. - NextGen Healthcare
Ambulatory-focused EHR/PM with patient portal and RCM options for small to enterprise practices; strong specialty content but variable learning curve across modules and integrations depending on legacy assets. - eClinicalWorks
Large cloud footprint, ambulatory and ASC-oriented offerings, patient engagement and telehealth built in; breadth can be an advantage, yet integration specifics and change management still require disciplined planning.
None of these is “perfect” for every practice. Many organizations adopt a commercial core and then commission custom ambulatory software development services to fill gaps—especially in AI agents, intake, analytics, and payer workflows.
Learn more: ➡️ How to Integrate Waystar with Custom Healthcare Applications
Why Many Providers Choose Custom Builds or AI Extensions
There are three recurring reasons organizations pursue custom ambulatory software development systems or hybrid extensions:
- Unique workflows and payer mix
Orthopedics, GI, behavioral health, or multi-site primary care often need rules that no vendor template anticipates. Custom ambulatory software development solutions let you encode local prerequisites (e.g., imaging before consult), particular order sets, or insurer quirks without waiting for vendor roadmaps. - Speed to value with agents, not monoliths
Adding AI agents around an existing EHR unlocks wins without a rip-and-replace: triage summarizers, benefit-explainers, or coding aides that sit in the message stream and staff queues. This is classic custom ambulatory software development services territory: small, governed services feeding your core. - Modernization of legacy systems
Many clinics run proven but aging PM/EHR stacks. A pragmatic path is to wrap them with modern APIs, an engagement layer, and AI services for transcription, summarization, and document extraction. Over time, you retire modules while keeping data continuity. - Open-source accelerators where they fit
Standards engines, such as HAPI FHIR, can anchor an interface layer; rule engines manage scheduling and referral prerequisites; open analytics stacks (e.g., dbt plus a BI tool) power custom ambulatory software development dashboards. This mix keeps you flexible. - Security and compliance posture
You control identity, auditing, and PHI boundaries. A custom gateway can enforce OIDC, consent checks, and payload scrubbing before any message reaches the EHR. That reduces surface area and keeps upgrades predictable. - Multi-system orchestration
Ambulatory rarely lives alone. Radiology, lab, ASC, and billing vendors change at different times. A custom orchestration layer stabilizes interfaces so front-end teams don’t chase every downstream change. - Measurement and continuous improvement
Off-the-shelf reports are good for snapshots, not hypotheses. A custom telemetry model ties show rates, auth delays, and payment conversions to interventions—nudge timing, message tone, or staffing. You iterate from evidence.
When you combine these ideas, custom ambulatory software development services become less about “reinventing an EHR” and more about adding intelligent glue: a governed layer of AI-assisted experiences, rules, and analytics that matches your practice’s reality and evolves on your cadence.
| Product | Core strengths | Common drawbacks | Integration and AI notes | Best fit |
|---|---|---|---|---|
| Epic (EpicCare Ambulatory) | Deep outpatient workflows; tight links across registration, orders, documentation, billing; strong data cohesion across service lines. | Complex governance; upgrade cadence can limit quick changes; higher staffing requirements for build teams. | Mature HL7 and FHIR; broad partner ecosystem; AI features growing yet often tied to enterprise governance. | Large health systems or multi-specialty groups that want a single, unified footprint. |
| Oracle Health (Cerner) Ambulatory | Cloud-forward suite; emphasis on interoperability and analytics; good coverage for ASC and clinic use. | Multi-product footprints may require careful interface mapping; change management can be time-consuming. | HL7, FHIR, and vendor tooling available; AI options exist but may require extra licensing and integration effort. | Health networks seeking a cloud path with strong connectivity and vendor services. |
| athenaOne (athenahealth) | Cloud EHR/PM with managed services; strong connectivity; growing AI assistants for documentation, scheduling, communications. | Template-driven workflows can feel rigid for niche specialties; reliance on vendor processes. | APIs and marketplace apps; AI available yet tuned to athena’s patterns. | Ambulatory groups that prefer a managed operating model with faster onboarding. |
| NextGen Healthcare | Ambulatory focus across small to enterprise practices; specialty content; portal and RCM options. | Learning curve varies by module; legacy integrations may add complexity. | Solid API and interface options; AI add-ons exist but may require partner solutions. | Specialty practices needing configurable content and RCM tie-ins. |
| eClinicalWorks | Large cloud footprint; ambulatory and ASC offerings; built-in patient engagement and telehealth. | Breadth brings variability; integration specifics and org change require disciplined planning. | FHIR and HL7 interfaces; partner add-ons for AI and analytics common. | Clinics wanting wide functionality in a single vendor stack. |
| Custom Ambulatory Solution | Workflow fit by design; pick web or mobile stacks that your team supports; selective modules for intake, scheduling, messaging, and custom medical billing software development; AI agents placed exactly where they reduce toil. | Requires strong product management, QA, and support; upfront discovery and integration work. | Full control over FHIR/HL7/X12, data contracts, and cloud or AI platforms; faster iteration on niche rules and payer logic. | Practices that want differentiation, tighter cost control over time, and the ability to extend quickly without waiting for vendor roadmaps. |
Ready to modernize your ambulatory system?
Layer a custom ambulatory platform over your existing systems: scheduling, digital intake, eligibility & claim status, patient payments on AWS, Azure, or GCP.
Step-by-Step Plan for Building Custom Ambulatory Software
- Define goals, scope, and KPIs: Meet with clinical leads, front desk, billing, and IT to capture pains and success metrics: no-show reduction; faster eligibility confirmation; quicker payment posting; shorter intake time. Prioritize a narrow MVP that proves value in 90 to 120 days.
- Choose build path: greenfield, upgrade legacy, or hybrid: If a legacy PM or EHR exists, wrap it with new engagement, scheduling, and billing services rather than replacing everything at once. A hybrid path reduces risk and cost, then you retire brittle modules after the new layer stabilizes.
- Select core standards and data contracts: Lock in FHIR R4 resources for Patient, Appointment, Coverage, Claim, and ExplanationOfBenefit, use HL7 v2 for ADT or ORM or ORU, and plan X12 flows for 270 or 271, 276 or 277, 837, and 835. Publish JSON schemas, define versioning, and set backward compatibility rules.
- Design identity, access, and consent: Adopt OIDC with OAuth 2.0, SSO for staff, and PKCE for mobile apps. Enable proxy access for caregivers and store consent snapshots with timestamps. If workforce features are in scope, plan SSO ties to custom HR software for healthcare for roles and time-based permissions.
- Draft the architecture blueprint: Favor a service-oriented design with an API gateway, identity, scheduling, intake, messaging, payments, and integration adapters. Use containers with Kubernetes or choose serverless for bursty workloads. Keep PHI boundaries explicit so services that touch PHI are isolated.
Pick the delivery stack: Web portals in React or Angular, or Vue, mobile apps in Flutter or React Native, backend services in Node.js or .NET, transactional storage in PostgreSQL or MySQL, caching in Redis, and object storage for documents. Centralize logs and metrics with ELK or OpenSearch plus Prometheus and Grafana. - Plan integrations first: Map EHR, PM, and clearinghouse touchpoints. Select an integration engine like Mirth Connect and add a FHIR server such as HAPI FHIR if the core system lacks one. Document message flows for scheduling, eligibility, claims, and remittance so that test cases are obvious.
- Embed AI where it removes toil: Use OCR or NLP for intake packet parsing and referral classification, summarization for message triage, and speech-to-text for notes. Platforms can include OpenAI or Azure OpenAI for language, Amazon Textract or Google Document AI, or Azure Form Recognizer for OCR. Align virtual visit features with patterns common to a custom telemedicine software development company.
- Sequence MVP features for fast wins: Start with eligibility at booking, rules-aware scheduling with waitlists, digital intake, two-way messaging, price visibility, and payment plans. Add telehealth hooks and education tracks in the next release, and defer RPM until workflows stabilize.
- Establish security and HIPAA posture: Use TLS 1.2 or higher, AES-256 at rest, least-privilege RBAC, immutable audit logs, standard BAAs, scheduled vulnerability scans, and a secrets manager. Define incident response and keep PHI-bearing services on segmented networks.
- Leverage open-source accelerators where it makes sense: Use HAPI FHIR for the FHIR layer, Keycloak for IAM, Mirth Connect for interfaces, dbt for data modeling, and Superset or Metabase for BI. If your practice includes in-house pharmacy or clinical research, borrow patterns seen in custom pharmaceutical software development services to manage auditability and validation.
- Set up development workflow and CI or CD: Use trunk-based development with pull requests and mandatory reviews, automate unit and integration tests in GitHub Actions or GitLab CI or TeamCity, and deploy with blue-green or canary strategies. Manage infrastructure as code with Terraform.
- Plan data migration and coexistence: When upgrading legacy, migrate demographics first, then scheduling, then billing artifacts. Run dual-write or near real-time sync during transition and keep reconciliation reports until cutover is complete.
- Test with realistic data and payers: Create synthetic datasets for protected test runs, validate X12 in clearinghouse sandboxes, run performance tests during peak hours, schedule UAT with front-desk and clinical super-users, and instrument the app for clickstream and error tracing.
- Execute go-live, training, and continuous improvement: Pilot at one site, track KPIs for one to two weeks, fix priority issues, then expand. Maintain a backlog for AI-agent refinements and new rules, and hold monthly ops reviews that connect metrics to changes.
Cost and Specialist Considerations
- Team composition (flex based on scope): product manager; solutions architect; clinical informatics specialist; backend engineers (Node.js or .NET); front-end web engineer; mobile engineer (Flutter or React Native); integration engineer (HL7, FHIR, X12); data engineer; AI/ML engineer for OCR and NLP use cases; DevOps; QA automation; security lead; UI/UX designer.
- Cost levers: reuse legacy where stable; adopt open-source for interfaces and FHIR; use serverless for spiky workloads; phase features; negotiate per-message pricing with clearinghouses; prefer managed databases to reduce on-call burden.
- Cloud choices: AWS (API Gateway, Lambda, RDS, Cognito or IAM Identity Center), Azure (API Management, Functions, Azure SQL, Entra ID), GCP (Cloud Run, Cloud Functions, Cloud SQL, Identity Platform). Select the cloud that your IT can support and where you can sign a BAA.
- AI platform choices: OpenAI or Azure OpenAI for general language tasks; Vertex AI or Bedrock for cloud-aligned governance; model monitoring via built-in observability or open-source dashboards.
This plan targets small to mid-sized ambulatory groups and medical centers: fast MVP, smart reuse of what you have, open-source where it saves money, and selective AI that reduces staff workload without disrupting clinical flow.
Conclusion: Get Your Custom Ambulatory Software Delivered
Custom ambulatory software works when it trims manual effort, clarifies scheduling and coverage, and connects clinical and revenue data through smart automation and AI. The playbook is straightforward: define measurable KPIs; add an engagement layer with FHIR, HL7, and X12 connectors; introduce AI agents for intake, triage, and billing explanations; then modernize legacy components in phases.
TATEEDA can guide each step with architecture, build, and custom software integration services that link EHR, PM, clearinghouses, and patient-facing apps into one coherent workflow. For added velocity, our nearshore software development services in the US pair U.S.-led delivery with cost-smart nearshore teams. Ready to move? Contact us to discuss your roadmap and get a practical estimate.





