How to Integrate AI into Healthcare Document Workflows

Slava Khristich



Vlad Nazarov
This guide shows how AI integration in healthcare document workflows moves from pilot to production: which documents benefit, what platforms to use, and how to wire everything into your EHR and revenue cycle with clear audit trails. It explains healthcare artificial intelligence implementation services for clinical documents that align with HIPAA, fits HL7 v2 and FHIR, and respect how clinicians work.
The market signal is loud. In 2023, U.S. entities reported 725 breaches involving 133+ million records; the operational and reputational cost makes automation and governance a survival topic, not a trend piece.
Then came the Change Healthcare incident, affecting ~192.7 million people, now the largest healthcare data breach on record. It began with a February 2024 ransomware attack, disrupted claims processing nationwide, exposed sensitive identifiers and treatment details, and forced months of recovery across providers and payers. HHS’ OCR later confirmed the $192.7 million figure, underscoring the importance of reducing human touchpoints, increasing validation, and maintaining airtight lineage.
Budgets back this shift. From 2019 to 2023, 75% of U.S. providers increased digital and IT budgets, and more than 85% expected further increases into 2024, with cybersecurity and workflow automation high on the list. Meanwhile, healthcare continues to generate a significant portion of the world’s data, with annual growth of nearly 36%, which compounds the documentation burden and makes scalable automation practical rather than optional.
Why TATEEDA is qualified to talk about AI workflow integration for patient engagement
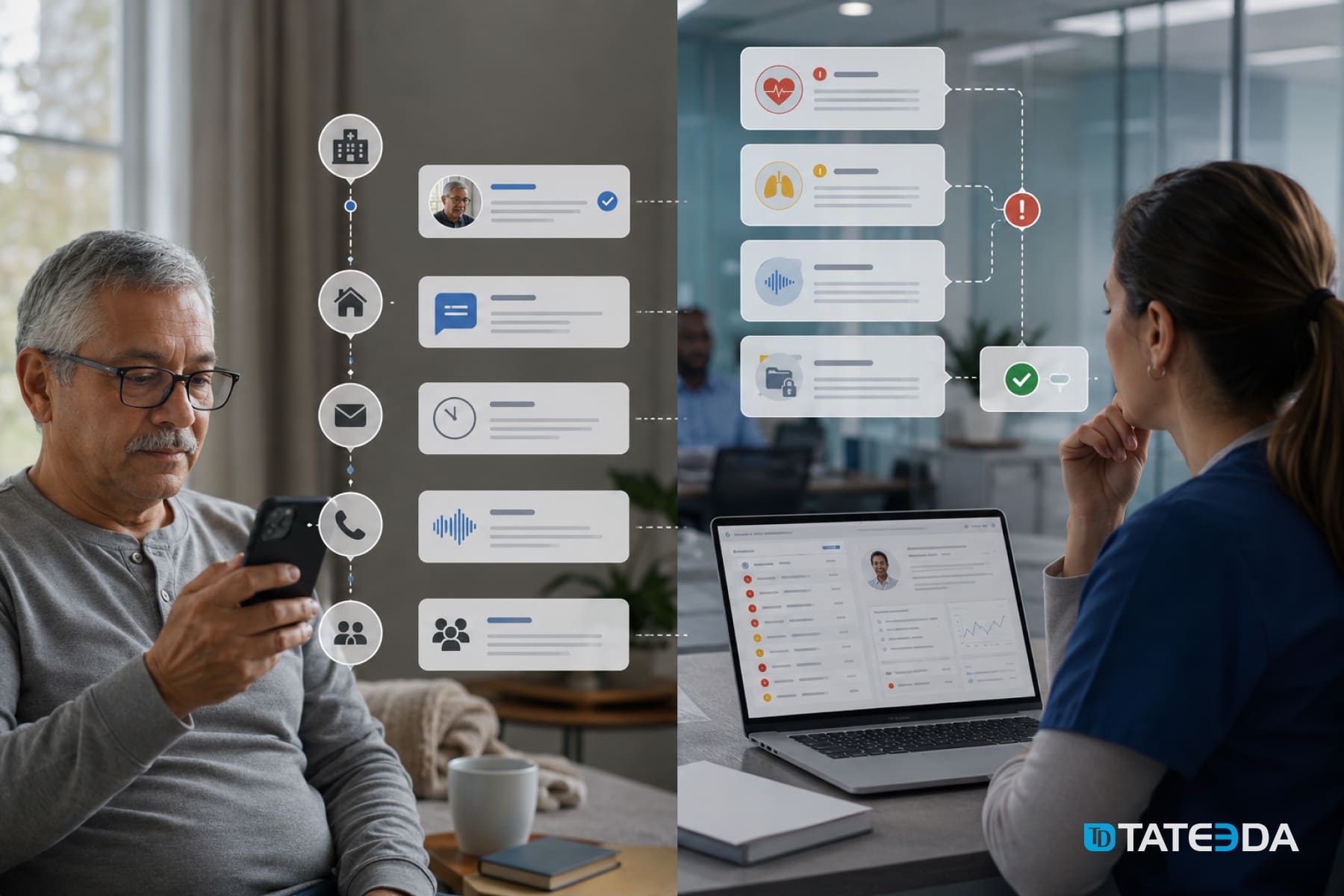
TATEEDA partnered with AYA Healthcare to build a multi-layer platform spanning patient and clinician portals, mobile apps, claim and payment integrations, and analytics. We added AI workflow integration: OCR and NLP for document intake, auto-classification of referrals and notes, field extraction mapped to FHIR R4 and HL7 v2, and X12 flows (270/271, 837/835). Identity runs on SSO and OAuth 2.0. Result: one experience for scheduling, credentialing, timesheets, and billing with fewer manual steps and a clear engagement timeline.
Beyond AYA, we provide custom healthcare software development services that include AI-assisted intake and consent, secure messaging, rules-aware self-scheduling, price transparency and payment plans, and outcome-linked education tracks. All follow HIPAA patterns with encryption, role-based access, and full audit trails, plus human-in-the-loop review for low-confidence extractions, data lineage, model versioning and monitoring, and clean EHR/EMR and RCM integration via FHIR APIs, HL7 v2, and X12.
Table of Contents
Types of Healthcare Documents that can be Integrated with AI
Document circulation in U.S. care is a relay: intake flows into orders, orders lead to results, results drive plans, plans trigger billing and reporting. Each step creates artifacts that must be read, validated, coded, routed, and then stored for audits. AI can classify, extract, reconcile, and post structured outputs into your clinical and financial systems without breaking existing processes.
Some document types where AI consistently helps:
- Patient intake forms: demographics, insurance, consents; normalize formats, auto-check completeness.
Consent forms: procedure, anesthesia, data-sharing; capture signatures and timestamps with OCR, verify required fields. - Progress notes: narrative text; sectioning plus NLP to surface problems, meds, allergies for quick review.
- History and physical (H&P): long narratives; parse problems and past procedures to accelerate clinician context.
- Orders and requisitions: labs, imaging, referrals; verify identifiers, orderables, priorities, and dates.
- Lab reports: chemistry, hematology, pathology; extract LOINC, values, units, reference ranges.
- Imaging reports: radiology narratives; pull impressions, critical findings, and follow-ups.
- Operative notes: procedures, devices used; suggest CPT candidates and implant specifics for validation.
- Discharge summaries: meds and instructions; reconcile lists, flag contradictions or duplications.
- Medication artifacts: e-Rx, MARs; validate drug, dose, route, frequency, duration.
- Prior authorization packets: multi-document bundles; assemble payer-specific fields, attach supporting notes.
- Insurance claims: CMS-1500, UB-04, 837/835; align documentation to codes, detect mismatches early.
- EOBs and remittances: denials and adjustments; match to claims, post write-offs, and create rework queues.
- Referrals and consult letters: reason for visit, urgency, attachments; route to scheduling with context.
- Audit and compliance artifacts: access logs, attestations; verify presence of required elements and retention metadata.
These classes map cleanly to EHR/EMR integration services with AI for document automation and support HL7/FHIR data extraction using AI in clinical workflows as you standardize inputs, outputs, and exceptions.

Learn more: ➡️ Hospital Management Software Development Services
Use Cases of AI Integrated with Healthcare Document Workflows
Chart Enrichment at the Point of Care
A clinician requests a six-month snapshot for complex patients. An AI-powered clinical document processing in healthcare service runs OCR on scanned consults, then applies section-aware NLP to progress notes, imaging reports, and discharge summaries. Output: a structured brief with problems, meds, allergies, and recent results that the provider can approve in seconds. Add a human-in-the-loop AI for the healthcare document validation step to keep quality high and leave a review trail for audits.
Prior Authorizations with Fewer Stalls
PA packets often stall on a missing detail. An agent classifies incoming artifacts, extracts payer-specific fields, and auto-fills forms; it pulls recent vitals, meds, and imaging via HL7/FHIR data extraction using AI in clinical workflows, flags gaps, and routes only the edge cases to staff. Framed within custom health insurance software development practices, this reduces back-and-forth, speeds determinations, and preserves a clear documentation history.
Revenue Cycle with Provenance
Denials tied to documentation gaps get expensive. An AI pipeline aligns each billed line to supporting chart text, highlights missing elements before submission, and reads EOBs to post adjustments or rework queues. This is AI-driven medical billing and claims document workflows with auditability and data lineage in AI-enabled healthcare documents, and it fits naturally into custom medical billing software development, so finance leaders can show exactly which sentence justified each code.
Fax-to-EHR Intake and Identity Matching
Many organizations still receive referrals, orders, and consult notes by fax or scanned PDFs. An intake service uses OCR and NLP for clinical document processing to classify document type, extract patient demographics, and detect order intent. It then runs identity resolution against an MPI using probabilistic matching and FHIR Patient $match, creates or links the Patient, and posts the artifact to the EHR via HL7 MDM or FHIR DocumentReference. Ambiguous matches route to a human-in-the-loop queue. Outcome: fewer orphan documents, faster indexing, and cleaner charts.
Care Coordination and Referral Loop Closure
After a referral is sent, closing the loop depends on receiving the specialist’s note and anchoring it to the originating order. An AI agent watches inbound documents, identifies consult letters, and attaches them to the correct encounter. It extracts assessment and plan, updates care gaps, and notifies the referring clinician. With EHR/EMR integration with AI for document automation, it writes structured findings to FHIR resources (ProblemListItem, Observation, MedicationRequest) and timestamps the loop closure for quality programs. Patients see status updates in portals or via custom patient engagement software, receive timely reminders and prep instructions, and coordinators spend less time chasing documents.
Quality Reporting and HEDIS Abstraction Acceleration
Quality teams manually abstract measures from notes, labs, and immunization records. An AI pipeline reads clinical narratives and lab reports, normalizes units, maps results to LOINC and SNOMED CT, and assembles numerator or denominator evidence for measures like A1c control or colorectal cancer screening. Outputs land in a governed store with auditability and data lineage that links every abstracted field to a page coordinate and model version. Reviewers validate exceptions through a lightweight UI, turning the system into an artificial intelligence implementation for clinical documents that reduces abstraction effort while preserving defensibility for audits.
| Use Case | Claims, encounter notes, coding sheets, EOBs, and remits | How AI Moves the Work | Standards & Impact |
|---|---|---|---|
| Chart Enrichment at the Point of Care | Unit normalization, code mapping to LOINC and SNOMED CT, and measure evidence assembly | Layout OCR, section detection, clinical entity extraction, compact briefing with confidence scores | FHIR writes to Problem, MedicationRequest, Observation; faster chart review, fewer missed details |
| Prior Authorizations with Fewer Stalls | Payer forms, clinician notes, imaging findings, vitals snapshots | Document triage, payer-field extraction, auto-fill, gap spotting, exception routing | FHIR pulls; HL7 v2 for results; X12 278 where used; shorter PA turnaround, fewer resubmissions |
| Revenue Cycle with Provenance | Line-to-note linking, compliance checks, denial reason parsing, and pre-submission validation | Referrals, orders, and consult letters arriving as fax or PDF | X12 837/835; HL7 MDM for updates; higher first-pass yield, reduced preventable denials |
| Fax-to-EHR Intake and Identity Matching | Scanned consults, progress notes, imaging reports, and discharge summaries | Classification, demographics extraction, order intent detection, probabilistic MPI match, human review for low confidence | FHIR Patient $match; HL7 MDM and FHIR DocumentReference; fewer orphan docs, faster indexing |
| Care Coordination and Referral Loop Closure | Inbound consult letters, follow-up notes, plan updates | Inbound consult letters, follow-up notes, and plan updates | FHIR updates to ProblemListItem, Observation, MedicationRequest; quicker loop closure, better gap closure |
| Quality Reporting and HEDIS Abstraction Acceleration | Clinical narratives, lab panels, immunization records | Consult detection, plan extraction, care-gap reconciliation, and provider notifications | FHIR Observation bundles; governed evidence store; fewer abstraction hours, audit-ready lineage |
Ready to Integrate AI with Healthcare Document Workflows?
Our team can scope, build, and launch a HIPAA-ready pilot quickly.
AI Platforms that Integrate with Healthcare Document Circulation
Below are active, widely used options that support OCR/NLP pipelines, custom extraction, and API-friendly outputs. Each can be deployed within HIPAA-eligible services under a Business Associate Agreement.
Microsoft Azure AI Document Intelligence
Prebuilt models for forms and IDs plus custom extractors; strong layout capture, handwriting support, selection marks, and table parsing. Outputs JSON with bounding boxes for downstream validation UIs. Azure services offer HIPAA BAA eligibility; confirm your in-scope services and sign a BAA before processing PHI.
AWS Textract + Amazon Comprehend Medical
Textract handles text, key-value pairs, and tables from scans and PDFs; Comprehend Medical extracts clinical entities like medications and diagnoses. Both are HIPAA-eligible services; route outputs through VPC endpoints and PrivateLink for tighter network control.
Google Cloud Document AI + Vertex AI Search for Healthcare
Document AI provides parsers for general and healthcare documents; Vertex AI Search for Healthcare can index FHIR R4 data to support chart search use cases. Both run within Google Cloud’s HIPAA program under a BAA when configured correctly.

A Step-by-step Integration Algorithm (Technical)
- Define outcomes and policies: pick 1–3 document types, set KPIs (turnaround time, exception rate, cost per doc), and specify PHI handling, retention, access controls, and encryption. Align to HIPAA Security and Privacy Rules; decide which workloads stay in VPC or on-prem.
- Sample and label: gather 200–500 real samples per class; label 15–30 fields that matter; capture variance (templates, stamps, handwriting, fax noise). Store with dataset versions and lineage.
- Choose engines: start with a cloud OCR/layout service; add custom extraction where prebuilt models miss target fields; for narratives, add clinical NLP. Select only HIPAA-eligible services and execute BAAs before using PHI.
- Define schemas: map outputs to internal objects and standard terminologies where possible (ICD-10, SNOMED CT, LOINC). For interoperability, map to FHIR R4 resources such as Patient, Encounter, Observation, MedicationRequest.
- Assemble the pipeline: ingest (S3, Blob, GCS, SFTP, API), classify, OCR, extract tables and key-values, run NLP, score confidence, route exceptions to a review UI, post JSON to queues or FHIR endpoints.
- Wire to clinical and RCM systems: use HL7 v2 messages (e.g., ORU for results) through your integration engine, and FHIR APIs per the ONC Cures Act requirements for certified API technology; secure with OAuth 2.0 and TLS 1.2+.
- Human-in-the-loop: build a validation station that shows each low-confidence field with its source snippet and coordinates; every correction flows back to the training set. This operationalizes human-in-the-loop AI for healthcare document validation.
- Security and auditing: encrypt in transit and at rest, segment roles, and write immutable logs that link every output field to model version and page coordinates. This enables auditability and data lineage in AI-enabled healthcare documents and speeds dispute resolution.
- Acceptance criteria: define field-level thresholds; e.g., MRN ≥ 98%, service date ≥ 97%, total charges ≥ 95%. Track precision/recall per field and per document class.
- Release engineering: maintain dev, test, and prod; use feature flags to roll out by facility or document type; keep rollback plans.
- Monitoring and retraining: watch drift, queue depths, and exception rates; retrain custom models when drift crosses thresholds; version models and datasets with change logs.
- Program governance: register models, datasets, policies, and approvals; keep evidence for HIPAA audits and ONC HTI-1-related inspections.
Conclusion: How We Help with AI-enhanced Workflows
AI integration in healthcare document workflows is no longer a side project, it is the connective tissue that steadies intake, charting, referrals, prior authorization, and billing. The playbook is clear: use OCR and NLP to read mixed formats, extract fields with confidence scores, route edge cases to a human reviewer, and post structured outputs through HL7 v2, FHIR R4, and X12. Add auditability and data lineage so every value traces back to a page and model version, respect HIPAA with encryption and access controls, and select platforms like Azure AI Document Intelligence, AWS Textract with Comprehend Medical, or Google Document AI that fit your environment. The payoff shows up everywhere: faster clinical decisions, closed referral loops, fewer denials, cleaner compliance checks.
TATEEDA can help you move from idea to production. Our team plans architectures, integrates EHR and RCM systems, builds validation UIs, and hardens pipelines for HIPAA. We have delivered patient portals, claims and eligibility flows, HL7 and FHIR exchanges, and AI-assisted intake for U.S. providers. Tell us your target documents and success metrics, and we will design a phased rollout that delivers quick wins first, then scales across sites. Ready to reduce manual touchpoints and raise confidence in every record? Let’s scope your next step.
FAQ: Artificial Intelligence in Clinical Documentation
What is AI-powered clinical document processing in healthcare?
It is the end-to-end use of OCR and NLP to classify, extract, validate, and route data from unstructured artifacts like referrals, notes, lab reports, and EOBs. With AI-powered clinical document processing in healthcare, outputs are posted as structured JSON or mapped to FHIR resources, then written into EHR or billing systems with confidence scores and exception queues.
How does artificial intelligence implementation for clinical documents connect to our EHR and lab systems?
Artificial intelligence implementation for clinical documents plugs into your stack through EHR/EMR integration with AI for document automation, using HL7 v2 messages for legacy interfaces and FHIR R4 APIs for modern apps. Typical flows include HL7 MDM and ORU, plus FHIR DocumentReference, Observation, and MedicationRequest. For labs and imaging, the pipeline augments orders and results with HL7/FHIR data extraction using AI in clinical workflows.
Which specialists do we need for a successful rollout?
Plan for a cross-functional pod: product manager, solution architect, integration engineer (HL7 v2 and FHIR), ML engineer, data engineer, MLOps, back-end engineer, front-end engineer for the reviewer UI, QA automation, DevSecOps, and a security or compliance lead. For scale, add a data steward to maintain ontologies and a clinical SME to tune human-in-the-loop AI for healthcare document validation.
What are typical timelines and costs?
A realistic outline:
- Discovery and technical spike (2–4 weeks): dataset audit, target fields, security plan, POC of OCR and NLP for clinical document processing. Rough cost: 25–60k USD.
- Pilot on 1–2 document classes (6–10 weeks): production-ready pipeline, reviewer UI, basic HL7 or FHIR integration. Rough cost: 90–220k USD.
- Scale-up to multiple classes and sites (3–6 months): advanced rules, analytics, auto-retraining, full RCM integration. Rough cost: 250–800k USD.
Drivers: document variance, EHR connectivity, security requirements, volume, and the share of custom extraction vs prebuilt models.
How do we keep it HIPAA-compliant and auditable?
Use HIPAA-eligible services under BAAs, encrypt in transit and at rest, isolate PHI within VPCs, and enforce least-privilege roles. For provability, store source page coordinates, model version, and reviewer actions so you have auditability and data lineage in AI-enabled healthcare documents. Add redaction for non-required PHI, plus monitoring that alerts on unusual access patterns.
What outcomes should we expect after go-live?
Teams typically see 30–60% less manual entry for targeted documents, 20–40% faster prior authorizations, and 10–20% fewer preventable denials once the loop between extraction and coding is closed. Since you are running AI-powered clinical document processing in healthcare with exception review, accuracy climbs over time as corrected fields feed back into retraining.