AI Medical Practice Software: How to Build an ERP System That Scales

Slava Khristich



Vlad Nazarov

In this article, we explain why AI medical practice software works best on a unified ERP foundation, which AI modules tend to bring the strongest operational return, how HIPAA, PHI, and BAA requirements shape the technical architecture, how FHIR-based EHR, billing, and device integrations fit together, and what build timeline and budget range practices should realistically expect.
Building AI medical practice software starts with a clear architecture decision: you need a unified Enterprise Resource Planning (ERP) system that connects scheduling, billing, clinical documentation, HR, and analytics under one data layer, and then layers machine learning across each module to automate the decisions your staff currently make manually.
| Real-World Scenario: Dr. Rachel Kim runs an eight-physician orthopedic group in Phoenix. Her practice uses five separate tools: a scheduling platform, a standalone Electronic Health Record (EHR) system, a third-party billing vendor, a payroll system, and a spreadsheet for medical supplies. None of them shares data. The AI scheduling feature she pays extra for was trained on hospital inpatient data, useless for an outpatient orthopedic workflow. Every month, roughly $31,000 in denied claims lands in her team’s queue, half of it preventable if someone had checked payer rules before submission. Three full-time staff members handle prior authorizations manually. Patients wait 48 hours to confirm appointments that should be confirmed in two minutes. |
Dr. Kim’s practice doesn’t have a software problem. It has a fragmentation problem. And AI can’t fix fragmentation; it needs integration first.
This guide covers the architecture and compliance blueprint for AI medical practice software development, specifically for practices with five to 50 providers that have outgrown simple scheduling-plus-billing tools but are not hospital systems. You’ll get the AI module breakdown, Health Insurance Portability and Accountability Act (HIPAA) compliance requirements for AI inference pipelines, an EHR integration design, a seven-step development process, and realistic cost data by module.
| Key Takeaways ➡️ AI medical practice software requires a unified ERP foundation first; machine learning applied to fragmented tools produces fragmented results. ➡️ Six AI modules drive the highest ROI for medical practices: predictive scheduling, ambient clinical documentation, automated CPT/ICD coding, denial prediction, inventory intelligence, and practice analytics. ➡️ Only 23% of health systems have Business Associate Agreements (BAAs) in place with their AI vendors, a HIPAA exposure most practices don’t know they’re carrying. ➡️ Protected Health Information (PHI) must never pass through third-party AI inference endpoints without a signed BAA, a de-identification layer, or both. ➡️ The $3.20 return per $1 invested in healthcare AI, realized within 14 months on average, applies specifically when AI runs on a unified data layer, not stacked on disconnected point solutions. |
Table of Contents
Practice Management Software vs. Medical ERP: Which Does Your Practice Need?
The terms get used interchangeably. They shouldn’t be.
Medical practice management software handles the front-office layer: scheduling, appointment reminders, basic billing, and patient registration. It’s designed for solo practitioners and small clinics. The data model is shallow, including patient demographics, appointment slots, insurance IDs, and claim submissions. That’s sufficient for a two-physician primary care office.
A medical ERP goes deeper. It unifies back-office operations: supply chain, HR and credentialing, financial reporting, compliance documentation, and clinical workflow automation alongside front-office functions. The structural difference is the shared data layer.
Every transaction in scheduling touches the financial module. Every CPT code submitted affects the denial analytics module. AI becomes useful when it can see the full operational picture.
Five operational signals that indicate ERP readiness
Your practice needs a full medical ERP when you recognize at least three of these conditions:
- Multiple locations or specialties sharing one billing entity but running separate scheduling workflows
- Staff count exceeding 25–30, where HR compliance, credentialing, and time tracking require dedicated management
- Denial rate above 8–10%, indicating billing and clinical documentation are disconnected
- Monthly administrative overtime paid because staff cannot complete core workflows within normal hours
- Reporting requires manual data pulls from two or more systems every week.
If that list describes your practice, patching another point solution onto your existing stack compounds the problem. You’re adding another data silo, not reducing them.
The hidden cost of patching tools together
Integration fees between point solutions add up faster than most practices realize. A typical practice paying separately for a practice management system, an EHR with a bolt-on AI layer, a billing clearinghouse, and a payroll platform pays for four integration maintenance contracts, and still gets data that arrives in different formats, on different schedules, and with different identifiers for the same patient record.
| Cautionary Case: An IT director at a 14-location family medicine group in Texas spent $240,000 customizing a commercial healthcare ERP over two years to handle their specific shift rotation rules and Texas Medicaid billing nuances. The off-the-shelf AI features were trained on commercial payer data sets from hospital systems, irrelevant for their patient mix. After two years, they were still managing provider scheduling in Excel. When our engineers audited their architecture in early 2025, the gap analysis showed a custom ERP build would have cost $180,000 and given the practice ownership of both the data model and the AI training corpus from day one. |
Our general healthcare ERP implementation guide covers the broader landscape of ERP types and deployment options. This article focuses specifically on the AI architecture decisions that separate a genuinely intelligent practice system from a traditional ERP with AI branding.
AI Module Architecture for a Medical Practice ERP
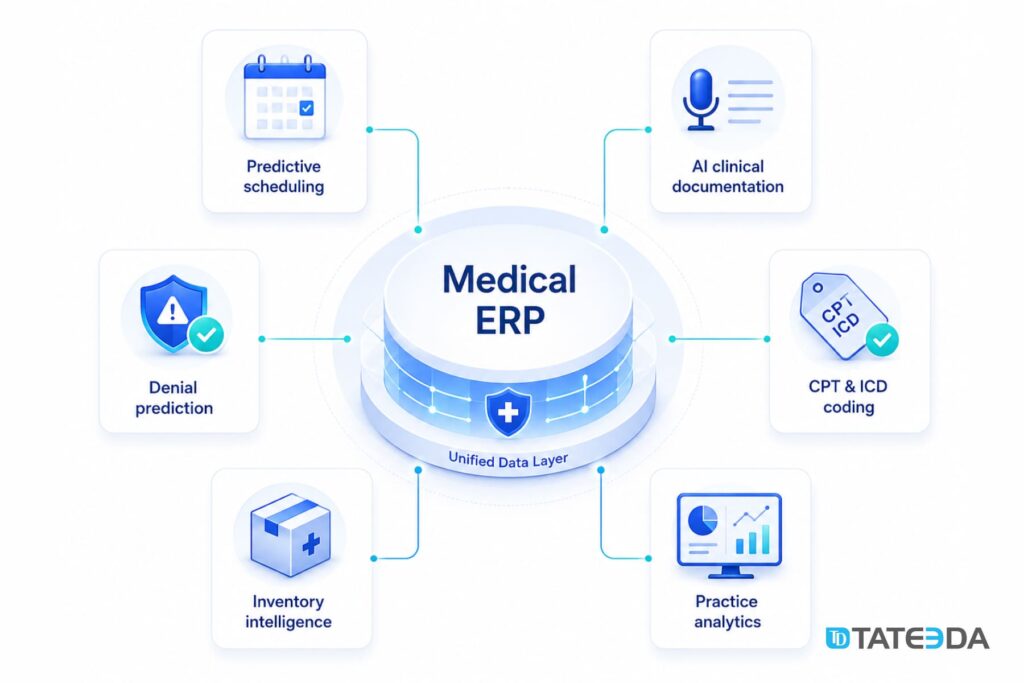
The right AI modules for a medical practice depend on where administrative overhead is highest. For most practices between 10 and 50 providers, six modules account for 80–90% of the automatable workload.
Predictive scheduling and no-show prevention
A scheduling AI model trains on historical appointment data: procedure type, provider, patient demographics, insurance type, day of week, and seasonal patterns. Within six to eight weeks of production data, the model predicts no-show probability per appointment slot with 75–85% accuracy in most practice configurations.
The practical output: high-risk slots get double-booked automatically. Premium low-risk slots stay single-booked. Patient reminder cadences adjust based on individual predicted behavior rather than a one-size-fits-all schedule. Practices implementing this approach typically see no-show rates drop from 18–22% to 8–11%.
AI-assisted clinical documentation
Ambient clinical documentation converts physician-patient conversation into structured clinical notes in real time. The technology stack: a lightweight speech-to-text layer (Azure Cognitive Services or AWS Transcribe Medical work well in BAA-covered environments), followed by a clinical Natural Language Processing (NLP) model that maps transcribed text to structured fields in the EHR.
The result is edited structured notes rather than notes typed from scratch. Documentation time drops 35–45% in typical deployments. The physician reviews and signs; the AI drafts. This matters for ERP integration because documentation velocity directly affects billing cycle speed and provider capacity.
Automated medical coding
CPT and ICD-10 code generation from clinical notes is one of the most mature AI applications in medical practice software development. Modern models achieve 95–98% coding accuracy in practices with consistent documentation standards.
The integration architecture: the NLP module that processes clinical notes pipes structured output to the coding model, which suggests CPT/ICD combinations ranked by confidence score. A human coder reviews the top suggestion and approves or overrides. Coding time drops roughly 40% per encounter in practices with mature AI coding implementations.
This is where EHR integration quality determines the AI’s accuracy ceiling. Sparse or inconsistent clinical note structure produces inconsistent coding suggestions. The EHR and the coding AI must share the same clinical data schema.
Revenue cycle AI: denial prediction and prevention
Denial prediction runs as a pre-submission claim scrubbing layer. The model trains on your historical denial data, broken down by payer, CPT code, diagnosis combination, provider NPI, and authorization status. Before a claim submits to the clearinghouse, the model scores it for denial probability.
Claims scoring above the threshold route to a human reviewer. Claims scoring below it submit automatically. In a practice with 1,000 monthly claims and a 15% denial rate, routing 10% of claims through human review, the highest-risk ones, cuts rework volume by 40–60%. If each denied claim costs $25–$40 in rework labor, preventing 100 denials per month saves $2,500–$4,000 monthly before counting the revenue acceleration from faster collections.
Our HIPAA-compliant healthcare software development teams build denial prediction as a standalone microservice that connects to existing clearinghouse integrations, no full ERP replacement required if denial prediction is your first priority.
Inventory and supply chain intelligence
For practices with in-house procedure suites, imaging, or lab operations, supply chain AI tracks consumption patterns against the appointment schedule and auto-generates purchase orders when inventory drops below dynamically calculated par levels. The model accounts for seasonal demand variation, supplier lead times, and procedure mix changes.
The integration touchpoint: the scheduling module feeds expected procedure volumes into the supply forecasting model weekly. The ERP’s purchasing module receives auto-generated requisitions. Manual inventory counts drop to exception handling rather than routine work.
Predictive analytics dashboard
The analytics layer aggregates data across all modules and surfaces operational signals: provider utilization rates by day and procedure type, revenue-per-encounter trends by payer, no-show cost attribution, and supply variance from budget. The AI layer adds predictive capability, forecasting revenue 30, 60, and 90 days out based on current scheduling fill rates and payer mix.
This module is the one most practices want to start with. It’s also the one that requires the most foundation work. Predictive analytics is only as accurate as the data it reads. If scheduling, billing, and clinical documentation still live in separate systems, the analytics layer produces averages, not actionable intelligence.
HIPAA Compliance Architecture for AI-Powered ERP
AI introduces HIPAA exposure that most practices haven’t fully mapped. The HHS HIPAA Security Rule covers PHI in all electronic forms, including PHI used as AI model training data and PHI processed by AI inference endpoints.
PHI handling in AI inference pipelines
Every AI module in your ERP that processes PHI touches the HIPAA compliance layer. The common failure mode: a practice integrates a cloud-based AI coding or documentation service without a signed BAA. The AI vendor processes PHI. That’s a HIPAA violation regardless of how capable the product is.
Three compliant architecture options:
- BAA-covered cloud inference: Use AI services from vendors that sign BAAs and maintain HIPAA-eligible infrastructure. AWS HealthLake, Azure Health Data Services, and Google Cloud Healthcare API all support this. Every AI endpoint PHI touches must fall within a BAA boundary.
- De-identified data pipeline: Strip PHI before sending data to any AI service that lacks a BAA. Safe Harbor de-identification removes 18 specified identifiers. Expert Determination uses statistical analysis to verify re-identification risk. De-identified data is not PHI under HIPAA and can use any AI service.
- On-premises or private cloud inference: Deploy AI models within your own infrastructure boundary, where PHI never leaves your controlled environment. Higher cost; appropriate for large practices or those with specific regulatory requirements.
BAA requirements for AI/ML vendors
Only 23% of health systems have BAAs in place with their AI vendors. That statistic likely understates the exposure in smaller practices, where procurement decisions happen faster and compliance review is less systematic.
Every AI service your ERP touches, coding APIs, NLP services, ambient documentation tools, analytics platforms, requires a BAA if it processes PHI. The BAA defines what the vendor can do with the data, how long they retain it, and what their breach notification obligations are. Vendors that refuse to sign BAAs are not HIPAA-eligible partners, regardless of how they market themselves.
Build a vendor BAA checklist into your ERP procurement process. TATEEDA’s healthcare IT consulting team audits AI vendor BAA coverage as part of every healthcare ERP engagement, because the technical integration is meaningless if the compliance layer has gaps.
Audit logging and model explainability
HIPAA’s Security Rule requires audit controls that track access to PHI. For AI systems, that extends to logging which model version generated a coding suggestion, which user approved it, and what the source clinical data was.
For AI modules that influence clinical decisions, coding, documentation, risk scoring, explainability requirements are growing. The FDA’s AI/ML-Based Software as a Medical Device framework is relevant if any AI module crosses into clinical decision support territory. Know the regulatory boundary before you build it.

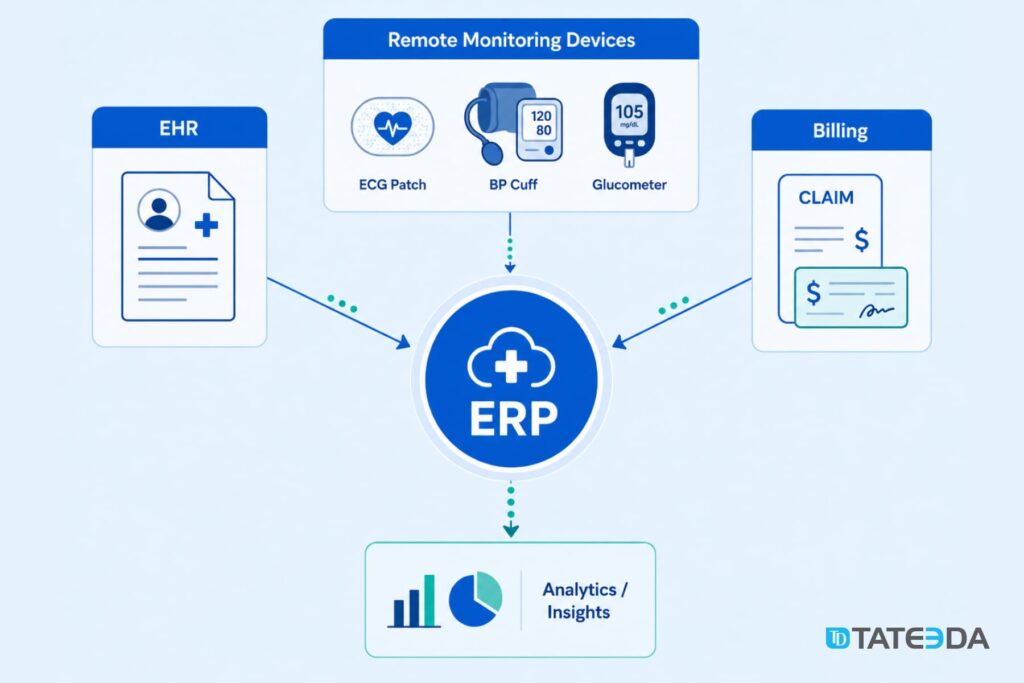
Integration Layer: Connecting ERP to EHR, Billing, and Devices
A custom medical practice ERP rarely replaces the EHR. More commonly, the ERP wraps around it: pulling clinical data for AI processing, pushing back coding suggestions and documentation drafts, and exchanging financial and scheduling data in real time.
FHIR R4 as the AI data pipeline
Fast Healthcare Interoperability Resources (FHIR R4) is the standard data exchange layer between your ERP and EHR. Every major EHR platform supports FHIR R4 with OAuth 2.0 and SMART on FHIR authorization.
The practical architecture: your AI coding module calls the EHR’s FHIR endpoint to retrieve the clinical encounter, processes it against the coding model, and writes the CPT/ICD suggestion back as a FHIR Task resource. The EHR renders it in the coder’s workflow with no manual copy-paste and no dual entry. The FHIR layer also powers the analytics module: patient demographics, encounter history, and diagnosis trends are queryable without building a separate data warehouse in year one.
Epic, Oracle Health, and athenahealth connector patterns
Epic’s FHIR API supports read operations broadly and write operations on a slower certification timeline. For Epic integrations, plan for a read-first architecture: your ERP reads clinical data via FHIR, processes it in your AI layer, and writes results back via Epic’s native API or a certified integration partner. Oracle Health (formerly Cerner) has a more open write API through its SMART on FHIR implementation. athenahealth supports both FHIR and proprietary API integrations through its Marketplace program.
Our EHR integration services cover Epic, Oracle Health, athenahealth, NextGen, and other major platforms, including the vendor certification processes some of these integrations require before going live.
IoT data ingestion for remote monitoring
Practices with remote patient monitoring programs, cardiac, respiratory, diabetes management, generate device data that belongs in both the ERP analytics layer and the billing layer. IoT sensor data from wearables, ECG patches, glucometers, and blood pressure cuffs requires a secure ingestion pipeline: HTTPS or MQTT transmission, a device data normalization layer, a FHIR Observation resource wrapper, and storage in your HIPAA-compliant data tier.
TATEEDA built the VentriLink remote cardiac monitoring platform, which handles real-time ECG data ingestion, arrhythmia detection, and physician event logging at clinical accuracy standards. That IoT development architecture informs how we design device data pipelines for medical ERP systems.

Before finalizing your technology stack, talk to our solution architects. The integration design decisions made in phase one constrain everything that follows. Schedule a technical consultation →
Build vs. Buy: When Custom AI ERP Beats Off-the-Shelf
SAP S/4HANA Health, Oracle NetSuite for Healthcare, and Microsoft Dynamics 365 Health are the dominant off-the-shelf options. All three can work for large health systems with significant IT departments to manage configuration and customization. For a 10–50 provider medical practice, the math often runs differently.
| Factor | Off-the-Shelf ERP | Custom AI ERP |
|---|---|---|
| Initial cost | $150K–$400K+ licensing + implementation | $120K–$300K development |
| AI customization | Pre-built models; limited training data control | Models trained on your specific patient mix and payer contracts |
| Payer-specific rules | Generic rule sets; manual customization required | Rules encoded from your own denial history |
| Integration flexibility | Certified integrations only; EHR write access limited | Custom FHIR connectors built to your EHR’s specific API version |
| Data ownership | Vendor-hosted; data export often contractually restricted | You own the data model and the AI training corpus |
| Ongoing costs | License escalation at renewal; per-seat pricing | Hosting + maintenance; no per-seat escalation |
| Timeline to go-live | 12–18 months with enterprise vendors | 8–14 months for full custom build |
The off-the-shelf AI ceiling for medical practices
The major ERP products were built for hospital systems and health networks with 500+ providers. Their AI features reflect that training history: optimized for DRG billing, calibrated for inpatient coding distributions, and configured for multi-facility supply chains. A 15-physician multi-specialty group has different coding distributions, different payer mixes, different no-show patterns, and different supply consumption profiles than a 300-bed hospital.
When you apply hospital-trained AI to a practice context, you get low-confidence coding suggestions, irrelevant denial prevention rules, and scheduling optimization that ignores your actual procedure mix. The AI needs to train on your data to be useful at your scale.
That doesn’t mean off-the-shelf is always the wrong choice. If your practice is standard, primary care, simple payer mix, single location, no procedure suite, a configured athenahealth or similar implementation may serve you adequately. The custom build ROI becomes compelling when you have complex billing rules, an unusual procedure mix, multi-location scheduling complexity, or specific compliance requirements (California’s PAGA and CCPA requirements, for example) that generic configurations handle poorly.
AI Medical Practice ERP Development: 7-Step Process
The following process applies to a custom AI ERP build for a practice of 10–50 providers. Timeline estimates reflect TATEEDA’s project data for practices with mixed-complexity EHR integrations.
- Operational audit and AI opportunity mapping (weeks 1–3): Document every manual workflow, identify the top five by time cost, and map the AI modules that address each. Define which modules go in phase one versus phase two.
- Data architecture and PHI classification (weeks 3–5): Design the core data schema. Classify every data entity by PHI status. Define encryption requirements, access control tiers, and FHIR resource mappings. This is the compliance foundation; shortcuts here create remediation costs later.
- EHR and billing system integration design (weeks 4–7): Map the FHIR API capabilities of your specific EHR version. Identify which data flows require FHIR read, which require write, and which require the EHR vendor’s proprietary API. Procurement of sandbox credentials and integration testing accounts happens in parallel.
- Core ERP module development (weeks 6–20): Build scheduling, billing, HR, and analytics modules on the shared data layer. AI hooks are scaffolded in but not yet populated with trained models. Go-live for the non-AI layer comes first, this is intentional, not a shortcut.
- AI model training and validation (weeks 16–26): Training data collection begins as soon as core modules are live and generating structured data. Minimum requirements: 90+ days of scheduling data for no-show prediction, 500+ coded encounters for coding model baseline accuracy, and 12+ months of claim history for denial prediction. Models train in parallel with core system operation.
- HIPAA security review and BAA procurement (weeks 18–24): Third-party penetration testing, BAA collection from every AI vendor in the stack, and Security Risk Analysis documentation (required under the HIPAA Security Rule). Plan four to six weeks for this phase. Compressing it creates compliance debt that surfaces during audits or after a breach.
- Phased rollout and model monitoring (weeks 24–36+): Roll out AI modules one at a time, starting with the lowest clinical risk (scheduling, coding suggestion review) before moving to higher-risk modules (denial prediction operating autonomously, supply auto-ordering). Monitor model accuracy metrics weekly for the first 90 days.
Total timeline from kickoff to full AI-enabled operation: 10–14 months for a complete build. A phase-one scope covering core ERP plus scheduling and coding AI delivers operational results in six to eight months.
Cost and Timeline Reality for Medical Practice ERP
Custom AI medical practice software development costs vary significantly by module scope, AI complexity, and EHR integration requirements. The following ranges reflect TATEEDA’s project data for practices in the 10–50 provider range.
Module-level cost estimates
| Module | Development Cost Range | Notes |
|---|---|---|
| Core ERP (scheduling, billing, HR, analytics) | $80K–$140K | Foundation layer; required before AI modules |
| Predictive scheduling AI | $25K–$45K | Training data from core ERP; 6–8 weeks post-launch |
| Clinical documentation NLP | $35K–$60K | Ambient recording integration adds complexity |
| Automated coding AI | $30K–$50K | Accuracy depends on EHR note structure quality |
| Denial prediction model | $25K–$45K | Requires 12+ months of historical claim data |
| Inventory intelligence | $20K–$35K | Simpler when procedure mix is stable |
| Analytics dashboard | $20K–$40K | Included in core ERP if architected early |
| Full build (all modules) | $180K–$300K | Timeline: 10–14 months |
These numbers assume a dedicated senior engineering team in TATEEDA’s hybrid delivery model: California-based architects and project managers, backed by pre-vetted senior engineers with healthcare EHR integration experience. We’ve built this kind of team for clients like AYA Healthcare, where AI-assisted development delivered a HIPAA-ready platform 4x faster than their previous timeline.
AI training data requirements and timeline impacts
The biggest timeline variable in AI medical practice software development is training data availability. If your current systems are fragmented, structured training data doesn’t exist yet. The core ERP must generate three to six months of clean, structured operational data before most AI models reach production accuracy.
Build this reality into your project timeline. Practices that try to skip the core ERP phase and bolt AI onto existing fragmented systems get exactly what they paid for: predictions based on incomplete, inconsistently formatted data that produces low-confidence suggestions and high override rates.
Use our custom software cost estimator to build a preliminary project budget for your specific practice configuration. It takes about five minutes and produces a scoped range you can bring into an architecture conversation.
Frequently Asked Questions
How long does it take to build a custom AI ERP for a medical practice?
A full build covering core ERP plus all six AI modules takes 10–14 months for a practice of 10–50 providers. A phase-one build covering core ERP plus scheduling and coding AI delivers results in six to eight months. Timeline depends primarily on EHR integration complexity and training data availability.
Can a small practice under 10 physicians justify custom AI ERP vs. off-the-shelf?
Rarely, unless the practice has unusual billing complexity, a procedure mix that off-the-shelf AI cannot model accurately, or specific state compliance requirements. For standard small practices, a well-configured off-the-shelf platform is more cost-effective. The custom build ROI improves significantly as provider count and transaction volume increase.
What AI modules deliver the fastest ROI for a medical practice?
Automated medical coding and denial prediction have the shortest payback periods, typically six to 12 months after go-live. Both reduce direct labor cost and accelerate revenue collection on claims that would otherwise sit in rework queues. Predictive scheduling follows, with measurable revenue impact within 12–18 months.
How does an AI ERP stay HIPAA-compliant when processing PHI for model training?
PHI used in AI model training must either be processed within a BAA-covered infrastructure environment or de-identified using Safe Harbor (18 identifiers removed) or Expert Determination methods before touching any AI service. De-identified data is not covered by HIPAA but cannot be re-identified. Every AI vendor in your stack requires a signed BAA if PHI enters their infrastructure.
How does a custom medical practice ERP integrate with an existing EHR system?
The standard architecture uses FHIR R4 APIs for bidirectional data exchange, authenticated via OAuth 2.0 and SMART on FHIR. Read operations (retrieving clinical data for AI processing) are broadly supported across Epic, Oracle Health, and athenahealth. Write operations (pushing coding suggestions and documentation drafts back) require vendor-specific API access or a certified integration partner. Your EHR’s specific version and API documentation determine which write methods are available.
Ready to Map Out an AI ERP for Your Practice?
Our solution architects will review your current tech stack, identify the highest-ROI AI modules for your practice, and give you a realistic build estimate.
Conclusion
AI medical practice software development delivers compounding returns when built on a unified data layer. The six AI modules with the clearest practice-scale ROI, predictive scheduling, ambient documentation, automated coding, denial prediction, inventory intelligence, and analytics, all depend on the same foundation: a custom ERP where every operational module shares a single structured data model.
The HIPAA compliance layer for AI is not optional and not simple. Every PHI-touching AI endpoint requires a Business Associate Agreement. De-identification and private infrastructure are the two compliant alternatives for endpoints that won’t sign BAAs. Build the compliance architecture before you build the AI models.
The seven-step development process outlines a 10–14 month path from operational audit to full AI-enabled operation. For most practices in the 10–50 provider range, the investment falls between $180,000 and $300,000 for a complete build, with a payback period of 10–14 months when denial prediction and coding automation reach production accuracy.
TATEEDA has built custom AI solutions for healthcare and ERP systems for medical practices, health systems, and health tech companies since 2013. Our team of 100+ senior engineers brings EHR integration, AI/ML, and compliance architecture experience to every engagement. We sign a BAA before writing a line of code.







