AI Healthcare CRM Development: Architecture, Features, and Patient Communications

Slava Khristich



Vlad Nazarov
In this article, we explain how AI healthcare CRM development works at the architectural level, including FHIR R4 EHR integration, real-time patient data synchronization, agentic AI patient-journey automation, HIPAA/CCPA compliance, and build-versus-buy decisions. You’ll also learn why clinical CRM systems need a data-first design, not a generic sales platform with healthcare features added later.
Effective AI healthcare CRM development combines a Fast Healthcare Interoperability Resources (FHIR) R4 real-time data layer, LLM-driven patient communications, and HIPAA-compliant audit infrastructure — built to match clinical data models, not adapted from general-purpose sales software.
Most health systems learn this distinction after a costly integration. A regional multispecialty group in California spent 18 months integrating Salesforce Health Cloud with their Epic environment. Their engineers built 14 custom middleware connectors to compensate for data model mismatches. Patient profiles were still 24 hours stale because the sync architecture relied on batch exports rather than real-time FHIR queries. Post-discharge communications failed 23% of the time — the automated outreach triggered before discharge status had propagated from Epic. The system was not broken. It was architecturally wrong for clinical use.
This article covers what a production-grade AI healthcare CRM requires at the architecture level: the FHIR R4 integration layer that keeps patient data current, the agentic AI workflows that automate patient journeys without human triggers, the compliance structure that California health systems need under both the Health Insurance Portability and Accountability Act (HIPAA) and the California Consumer Privacy Act (CCPA), and the build-vs-buy framework that determines which approach fits your organization’s scale and regulatory exposure.
| Key Takeaways: ✅ AI-native healthcare CRM development requires FHIR R4 real-time bidirectional sync with EHR systems — batch sync creates stale data that breaks clinical communications workflows. ✅ Agentic AI in patient relations means autonomous multi-step journey orchestration (post-discharge, care gaps, readmission risk) — distinct from chatbots and rule-based automation. ✅ CCPA’s right-to-delete creates direct architectural conflict with HIPAA’s six-year Protected Health Information (PHI) retention requirement; this must be resolved at the data model layer, not after deployment. ✅ Salesforce Health Cloud and Microsoft Cloud for Healthcare work for simple outreach use cases but require costly custom middleware for FHIR real-time sync, California dual compliance, and agentic AI orchestration. ✅ Custom AI healthcare CRM development typically costs $80,000 to $250,000+, depending on EHR integration scope, AI feature set, and compliance requirements. |

Why is TATEEDA qualified to tell you about AI in CRMs?
TATEEDA has been building healthcare software since 2013, including patient portals, medical mobile apps, payment systems, EHR-connected workflows, pharma automation platforms, and remote monitoring solutions. This gives our team direct experience with the data, compliance, and integration problems that make AI healthcare CRM development very different from ordinary sales CRM customization.
Our work sits at the intersection of healthcare architecture, patient communication, regulated data, and custom AI development. We understand why FHIR sync, PHI handling, audit logs, role-based access, human review, and HIPAA/CCPA data separation must be planned before AI features are added. That practical engineering background is why we discuss AI in healthcare CRMs from the system level: data model first, CRM logic second, AI orchestration after the foundation is safe enough to support it.
Table of Contents
What Is an AI Healthcare CRM? (Beyond the Feature List)
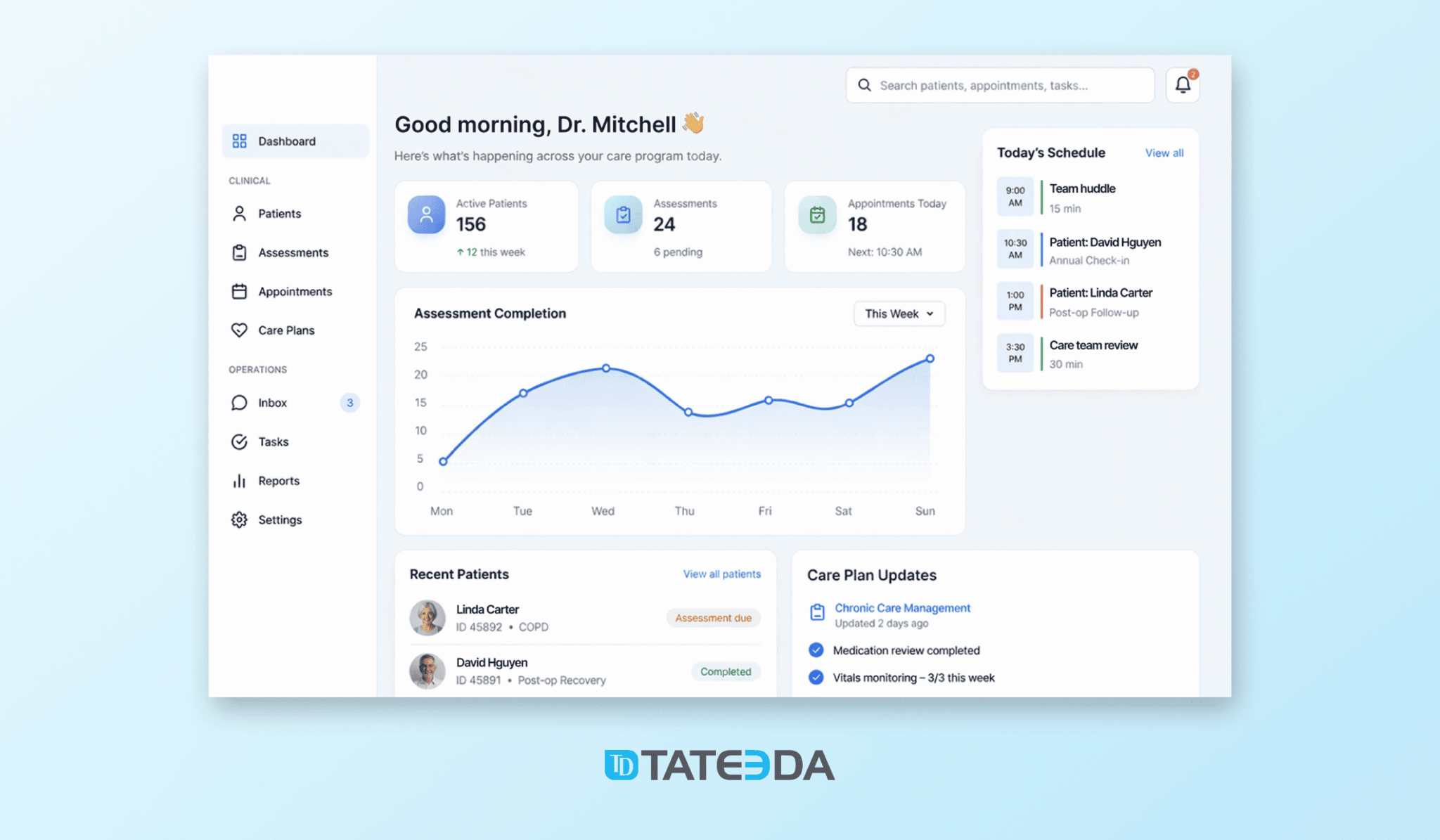
A healthcare Customer Relationship Management (CRM) system manages patient relationships across the full care continuum — from first contact and scheduling through care delivery, billing, and follow-up. The “AI” label is where most vendors blur the line between genuine capability and marketing language.
AI-native healthcare CRM development means the system’s core data model, communications logic, and workflow engine are designed from the ground up to use machine learning for segmentation, prediction, and autonomous orchestration. AI is not a reporting dashboard or a smart-send feature. It operates at the data layer.
Traditional CRM vs. AI-native healthcare CRM
Traditional healthcare CRM — including most Salesforce Health Cloud implementations — uses rules-based automation. If a patient has not scheduled a follow-up in 30 days, send a reminder. These systems are accurate when the rules are accurate and brittle when clinical context changes.
AI-native CRM replaces static rules with models. A post-discharge outreach system trained on 18 months of clinical outcomes learns that diabetic patients with HbA1c above 9.0 who live alone are significantly more likely to miss follow-ups, and adjusts both outreach timing and preferred channel accordingly. The system improves with each patient journey it processes.
The architectural difference matters more than the feature list. AI-native systems require:
- A real-time FHIR R4 data pipeline (not batch exports) that keeps the patient profile current as clinical events occur
- An embedding layer that converts clinical notes, diagnosis codes, and care plan status into features that the ML model can act on
- An event-driven communications engine that triggers outreach based on clinical state changes, not scheduled batch jobs
The Patient 360 model: where clinical and operational data meet
The Patient 360 model centralizes patient data from Electronic Health Record (EHR) systems, scheduling platforms, billing systems, and patient-initiated interactions into a single unified profile. In a custom AI healthcare CRM, this profile updates in real time via FHIR subscription resources — meaning the CRM knows a patient was discharged, prescribed a new medication, or flagged for a care gap within minutes, not the following morning.
This is the data foundation that every other feature depends on. An outreach engine operating on yesterday’s data is a clinical liability.
Core Features of a Custom AI Healthcare CRM
The feature set of a production healthcare CRM is well-documented in vendor materials. What receives less attention is the compliance and architecture requirements behind each feature.
AI-driven patient segmentation and predictive outreach
Patient segmentation in an AI healthcare CRM is dynamic. The model continuously re-scores patients based on updated clinical data: recent lab values, chronic condition status, appointment adherence, payer eligibility changes, and social determinants of health, where available. High-risk patients surface automatically for care coordinator review; low-risk patients receive automated touchpoints without staff intervention.
Predictive outreach in an AI patient engagement platform generates significant operational gains. AI-embedded CRM workflows reduce administrative workload by 30-40% in scheduling and patient access functions, according to research across large health system implementations (source: Strativera, 2025). For organizations with high patient volumes, this translates directly to reduced no-show rates and improved care gap closure — which, for value-based care organizations, affects quality measure performance and shared savings calculations.
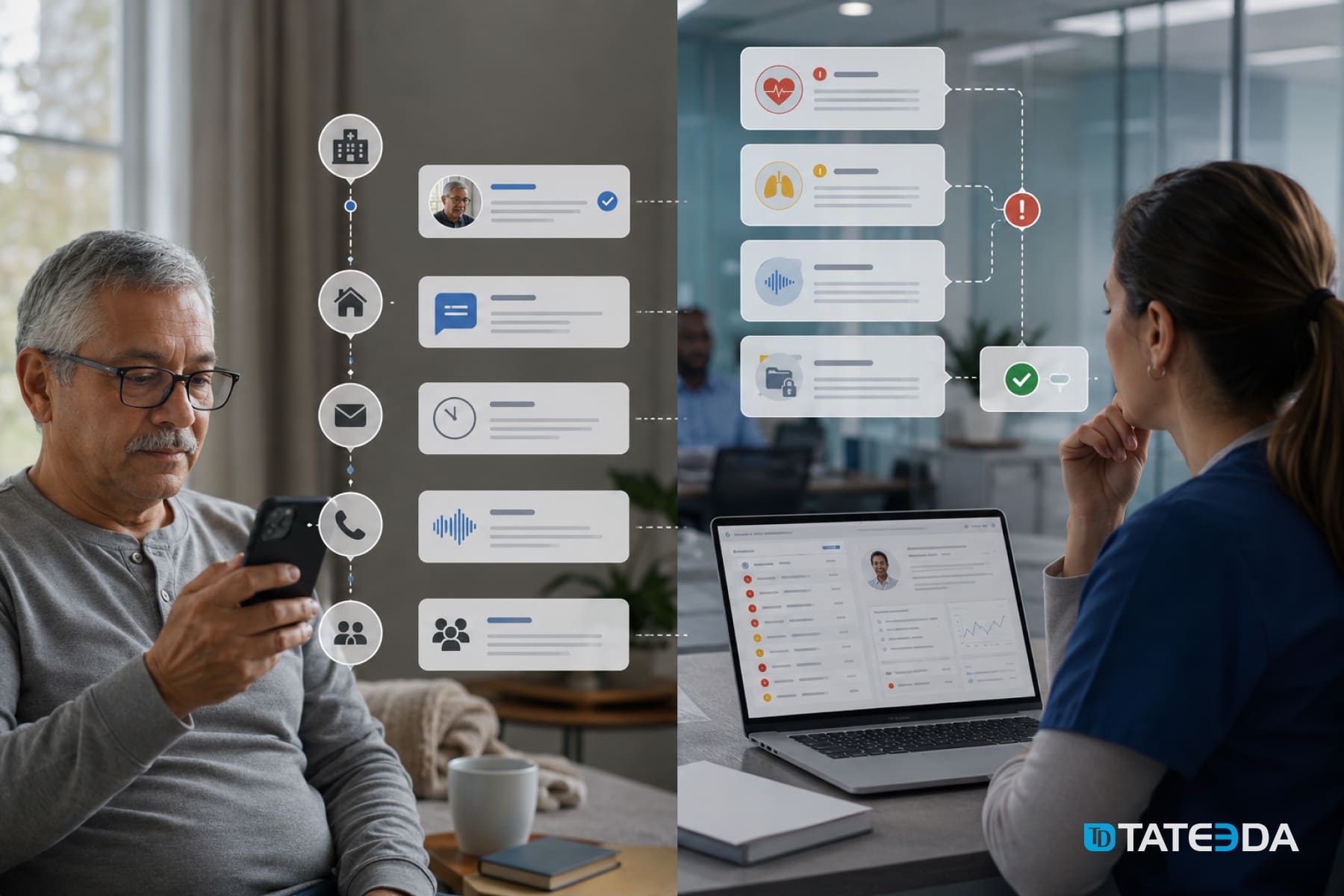
Omnichannel communications layer
Patient communications in 2026 operate across SMS, secure portal messaging, voice AI for phone interactions, push notifications via mobile health apps, and email for lower-acuity outreach. An AI healthcare CRM manages all channels from a single communications layer that respects patient channel preferences, opt-in/opt-out state, and preferred language.
HIPAA requirements differ by channel. SMS to patient-provided phone numbers for appointment reminders is permissible under the HIPAA Privacy Rule’s treatment exception. SMS containing clinical details requires explicit patient authorization. The communications layer must enforce these distinctions automatically, log every patient-facing communication with timestamps and channel metadata, and maintain records for a minimum of six years.
Voice AI in the outreach layer handles high-volume repeatable interactions — scheduling confirmations, prescription refill reminders, post-visit satisfaction surveys — without staff involvement. HIPAA-compliant voice AI vendors sign a Business Associate Agreement (BAA) and maintain zero-day data retention policies with underlying model providers to prevent PHI from entering training datasets.

EHR-synchronized patient profiles via FHIR R4
In a custom healthcare CRM, patient profiles sync bidirectionally with the EHR via HL7 FHIR R4 APIs:
- Clinical events in Epic, Oracle Health, or athenahealth immediately update the CRM patient profile via FHIR subscription resources
- Communications recorded in the CRM (appointment requests, patient-initiated messages, care coordinator notes) write back to the EHR encounter record
- Care plan changes in the EHR trigger communications workflows in the CRM without manual hand-offs
This bidirectional sync is what separates a clinically accurate CRM from a marketing automation tool with healthcare branding.
Care gap identification and proactive outreach
Care gap management — identifying patients overdue for preventive screenings, chronic disease management visits, or post-discharge follow-ups — is one of the highest-value applications of AI in a healthcare CRM. The system ingests claims data, clinical quality measures from the EHR, and payer-provided attribution data to identify patients with open care gaps, ranks them by risk and reachability, and initiates outreach workflows automatically.
For value-based care organizations, automated care gap closure directly affects HEDIS measure performance and shared savings distributions. This is not a nice-to-have feature. It is a revenue function.
HIPAA-compliant audit logging and consent management
HIPAA Security Rule requirements under 45 CFR Section 164.312(b) mandate hardware, software, or procedural mechanisms that record and examine activity in systems containing PHI. In a production healthcare CRM, this means:
- Every API call that reads or writes PHI is timestamped and attributed to a user or system identity
- Every patient communication is logged with content hash, channel, timestamp, and delivery confirmation
- Every consent change — opt-in, opt-out, channel preference update — is recorded with an effective date and source
- Logs are stored in append-only storage (not modifiable by application-layer operations) and retained for a minimum of six years
Consent management must also handle CCPA consumer data rights, which we address in the compliance section below.
Building a custom AI healthcare CRM?
TATEEDA’s medical CRM development services cover FHIR architecture, AI feature development, and HIPAA/CCPA compliance for US health systems.
FHIR EHR Integration for CRM: Why It’s the Most Critical Architecture Decision
The FHIR R4 integration layer determines whether a healthcare CRM operates on clinical reality or a stale approximation of it. Every AI feature in the system depends on the quality and latency of this data pipeline.
SMART on FHIR authorization in a CRM context
SMART on FHIR is the authorization framework governing how third-party applications — including a custom CRM — access patient data from an EHR system. It uses OAuth 2.0 with healthcare-specific scopes that define what resources an application can read or write, and on whose behalf.
A healthcare CRM connecting to Epic uses SMART on FHIR backend services authorization (server-to-server) for data sync. The CRM authenticates to Epic’s FHIR server using a JSON Web Token (JWT) signed with a registered private key. Epic validates the JWT, issues an access token, and the CRM’s FHIR client queries Patient, Encounter, Condition, MedicationRequest, and Appointment resources against that token.
The scopes requested determine what the CRM can access. A communications-focused CRM typically needs patient/Patient.read, patient/Condition.read, patient/Appointment.read, and patient/Appointment.write at minimum. Any scope that includes write access requires additional review in Epic’s App Orchard approval process.
Epic, Oracle Health, and athenahealth: integration patterns
The three major EHR platforms each expose FHIR R4 APIs with meaningful implementation differences that affect CRM development scope.
Epic: Exposes a mature FHIR R4 API with strong documentation. App Orchard review adds 4-8 weeks to initial integration timelines. Production access requires a signed BAA with Epic. Epic’s FHIR subscription resources support real-time notifications for Encounter and patient status changes — the mechanism that enables true real-time CRM sync.
Oracle Health (formerly Cerner): Uses Cerner FHIR APIs with OAuth 2.0, exposing a broad resource set. Real-time event streaming uses Cerner’s Ignite APIs. Organizations on Oracle Health Millennium require coordination with their health system’s integration team to enable third-party FHIR access.
athenahealth: Exposes FHIR R4 through the athenahealth Marketplace API. More accessible for smaller practices; Marketplace certification adds 6-10 weeks. Real-time sync relies on athenahealth’s webhook infrastructure rather than FHIR subscription resources.
Building integration connectors for all three platforms in a single CRM requires abstraction layers that normalize resource formats — a non-trivial engineering task that accounts for a significant share of custom AI healthcare CRM development cost. For organizations evaluating integration scope, TATEEDA’s EHR integration services cover Epic, Oracle Health, and athenahealth FHIR connector development.
Real-time vs. batch sync: what each use case requires
Not every CRM function requires real-time FHIR data. Batch sync via FHIR Bulk Export is sufficient for population-level analytics, care gap reporting, and weekly outreach campaigns. The operations that require real-time sync are those where clinical state changes must immediately affect communications:
- Post-discharge outreach (must not trigger before discharge status is recorded in the EHR)
- Appointment reminder cancellation when a patient reschedules in the EHR
- Medication adherence outreach synced to prescription dispensing events
- Escalation workflows triggered by abnormal lab results
Building both real-time and batch pathways into the FHIR integration layer — and routing each use case appropriately — is an architecture decision made at design time, not as a retrofit.
Agentic AI in Healthcare CRM: Patient Journey Automation at Scale
Agentic AI in the context of custom healthcare CRM software refers to an LLM-driven system that autonomously executes multi-step patient journey workflows, makes decisions about timing, channel, and message content based on current patient state, and escalates to human care coordinators when clinical judgment is required. This is the leading edge of the agentic AI patient journey model in 2026.
This is materially different from:
- Rule-based automation: If condition A, then action B. Brittle. Does not account for clinical context.
- Chatbots: Single-turn or limited-context conversational agents. Not able to orchestrate multi-day patient workflows.
- Workflow automation tools: Zapier-style step triggers without clinical reasoning capability.
What agentic AI does in patient relations
In a post-discharge follow-up scenario, an agentic AI system:
- Receives a FHIR Encounter resource indicating patient discharge from Epic
- Accesses the patient’s condition list, medication changes, and care plan from the EHR
- Determines the optimal first contact channel — a 72-hour portal message for patients with strong portal engagement history, or an SMS for patients with low portal utilization
- Drafts a personalized message referencing the specific discharge diagnosis and next care steps, within defined clinical safety guardrails
- Monitors for patient response; if no response arrives within 48 hours, escalates to a voice AI outbound call
- If the voice AI interaction surfaces concerning symptom language, it routes a care coordinator alert with full conversation context
The agentic system runs this complete workflow without a human initiating each step. Care coordinators review exceptions and escalations, not routine touchpoints.
The operational impact is measurable. Research published by PwC’s Health Research Institute documents readmission reduction of 15-20% in health systems deploying AI-driven post-discharge follow-up programs, compared to manual outreach workflows dependent on available staff capacity. Manual programs rarely achieve consistent outreach volume at scale.
Human-in-the-loop guardrails for clinical safety
HIPAA doesn’t prohibit autonomous AI-driven patient outreach, but it does require that PHI disclosed in outreach is the minimum necessary for the stated purpose. Clinical safety requires that agentic AI systems operate within defined content guardrails — a validation layer between the LLM output and the patient-facing message that checks content against clinical safety rules before delivery.
Messages that fail validation are held for care coordinator review. No autonomous AI system in a regulated clinical environment should deliver unapproved content directly to a patient without a human review checkpoint available.

HIPAA, CCPA, and California Dual Compliance in a Custom Healthcare CRM
For California-based health systems — and any organization serving California patients — HIPAA-compliant healthcare CRM development must satisfy two separate regulatory frameworks simultaneously. They conflict at a specific and important point. Organizations navigating this architecture decision benefit from TATEEDA’s healthcare software engineering services before committing to a data model.
HIPAA BAA requirements for CRM vendors
Under HIPAA, any party that creates, receives, maintains, or transmits PHI on behalf of a covered entity is a Business Associate. In a healthcare CRM deployment, this includes:
- The development firm building and hosting the system
- The cloud infrastructure providers (AWS, Azure, and GCP each offer HIPAA BAA coverage for specified services)
- Any AI/ML service processing PHI (OpenAI offers an enterprise API BAA; organizations must request it explicitly)
- Any voice AI vendor handling patient calls containing PHI
Every BAA must be executed before PHI enters the vendor’s environment. TATEEDA signs a BAA before writing the first line of code on any healthcare engagement.
CCPA patient data rights and the HIPAA retention conflict
The California Consumer Privacy Act (CCPA), as amended by the California Privacy Rights Act (CPRA), grants California consumers the right to request deletion of their personal information. A health system that receives a patient deletion request faces a direct regulatory conflict: CCPA mandates deletion; HIPAA requires PHI retention for a minimum of six years from creation or last use.
The legal resolution is explicit in California law. CCPA exempts information that a business must retain “to comply with a legal obligation” — which covers HIPAA’s six-year PHI retention requirement. This exemption applies only to the minimum PHI required for the legal compliance purpose. Non-clinical CRM data — marketing preferences, channel history, satisfaction survey responses — isn’t PHI and isn’t exempt from CCPA deletion.
A CCPA deletion request must, therefore, delete non-PHI operational CRM data while retaining PHI under the HIPAA carve-out. The CRM data model must maintain explicit separation between PHI fields and non-PHI operational data. Building this separation into the schema at development time costs two to three days of architecture work. Retrofitting it after receiving a California Privacy Protection Agency (CPPA) inquiry is a multi-week engineering engagement with legal risk attached.
Audit logging, data retention, and breach notification architecture
A compliant healthcare CRM maintains three infrastructure components that are distinct from application features:
Audit logs: Immutable, append-only records of all PHI access, modification, and patient-facing communications. Stored separately from application data with independent access controls. Retained for a minimum of six years. Not accessible to application-layer delete operations.
Data retention schedules: PHI retention governed by HIPAA at a minimum of six years. State-specific requirements apply where they exceed the federal floor. California imposes no PHI retention extension beyond HIPAA, though mental health records face additional state-level requirements.
Breach notification infrastructure: HIPAA requires covered entity notification to affected individuals and HHS within 60 days of discovering a breach involving PHI. The CRM’s security monitoring must detect anomalous PHI access patterns, generate incident alerts, and trigger documented response workflows. This is not a policy document — it is a technical monitoring and alerting system.

Build vs. Buy: Why Custom AI Healthcare CRM Development Outperforms Off-the-Shelf
The build-vs-buy decision in AI healthcare CRM development is not primarily a cost question. It is an architecture and compliance question. Cost is the consequence of answering those questions honestly.
Where Salesforce Health Cloud and Microsoft Cloud for Healthcare fall short
Salesforce Health Cloud is a capable platform for organizations with standard outreach needs, defined workflow requirements, and no real-time EHR sync requirements. It works well for patient intake management at outpatient practices, care management at smaller health plans, and appointment reminder campaigns driven by nightly data exports.
It encounters structural limits when organizations need:
- Real-time FHIR R4 bidirectional sync with Epic or Oracle Health (requires custom middleware that Salesforce does not provide natively)
- Agentic AI workflows with clinical context awareness (Einstein AI does not access EHR resources natively)
- California dual compliance with CCPA/PHI data segregation embedded in the schema
- Custom ML models trained on the organization’s own clinical and engagement history
The middleware cost to compensate for these gaps is high. Organizations that spend 12-18 months building adapters are often spending more than a custom CRM would have cost, while maintaining a complex integration layer they do not own.
When custom development is the right path
Marcus ran engineering at a 300-provider health system in Southern California. In 2024, his organization chose Microsoft Cloud for Healthcare over a custom build based on initial licensing cost. By month nine, his team had built 22 custom connectors to bridge Microsoft’s CRM data model with their Epic clinical workflows.
Every Epic update required connector maintenance. Their CCPA deletion process took four weeks of engineering time per request because the data model didn’t distinguish PHI from operational CRM data. The off-the-shelf system had become a bespoke integration project with a Microsoft licensing fee added on top.
Custom AI healthcare CRM development is the right choice when:
- The organization requires real-time EHR sync for clinically accurate patient communications
- Patient volume and care complexity make AI-driven segmentation a clinical necessity, not a convenience
- California CCPA compliance requires explicit data model segregation that off-the-shelf platforms do not provide
- The organization intends to build proprietary ML models on its own clinical and engagement data
- The 36-month total cost of ownership for a platform plus required customization exceeds the custom build estimate
Cost and timeline for custom AI healthcare CRM development
Custom AI healthcare CRM development typically falls in these ranges:
| Scope | Typical Cost | Timeline |
|---|---|---|
| MVP: single EHR integration, core communications, basic AI segmentation | $80,000-$120,000 | 4-6 months |
| Mid-tier: 2-3 EHR integrations, omnichannel comms, care gap workflows, AI segmentation | $150,000-$250,000 | 6-10 months |
| Enterprise: multi-EHR, agentic AI orchestration, CCPA/HIPAA dual compliance, custom ML models | $250,000-$500,000+ | 10-18 months |
These ranges reflect senior engineer rates for US healthcare-focused development. Generic offshore estimates in the $30,000-$50,000 range typically exclude FHIR integration complexity, compliance architecture, and the agentic AI layer — costs that surface later and inflate the final project spend.
How TATEEDA Builds AI-Native Healthcare CRM Systems
TATEEDA has delivered medical CRM software development and HIPAA-compliant patient-facing systems for health systems, digital health companies, and specialty practices since 2013. Our custom healthcare software development work covers the full stack — from FHIR integration layer through patient-facing communications and clinical workflow automation.
Our custom AI development for healthcare includes La Maestra Family Clinic, where we built an Android and iOS patient portal with a web admin in under one month, designed for a multilingual patient population with limited prior portal experience.
We also built a HIPAA-, NACHA-, and PCI-DSS-compliant patient payment portal for a multi-facility health system, with full audit infrastructure and immutable transaction logging. Both systems required the compliance architecture that off-the-shelf platforms can’t provide.
Our AI healthcare CRM development process:
- BAA signed before any PHI enters our environment
- FHIR integration architecture scoped first — the data layer determines every other capability
- Compliance requirements (HIPAA, CCPA, where applicable) designed into the schema before application development begins
- AI feature layer built on the data foundation, not added as a module at the end
- Dedicated development team integrated within 48-72 hours, attending your standups and shipping to your sprint cadence
Our 100+ senior engineers include architects with Epic, Oracle Health, and athenahealth integration experience. We don’t place junior developers on regulated healthcare projects.
Named to the Inc. 5000 four consecutive times (2022-2025), TATEEDA has built a track record in the exact intersection of engineering quality and regulatory compliance that healthcare CRM development demands.
Frequently Asked Questions
What is the cost to build a custom AI healthcare CRM?
Custom AI healthcare CRM development typically ranges from $80,000 for a focused MVP with a single EHR integration to $500,000+ for an enterprise system with multi-EHR integration, agentic AI orchestration, and full CCPA/HIPAA dual compliance architecture. The largest cost driver is the FHIR integration layer — real-time bidirectional sync with Epic, Oracle Health, or athenahealth requires significant engineering effort that generic offshore estimates routinely exclude.
How long does healthcare CRM development take?
A focused MVP with a single EHR integration and core AI communications features typically takes 4-6 months with a senior engineering team. Enterprise engagements with multi-EHR support and custom ML model development run 10-18 months. Organizations that compress architecture planning to reduce the timeline typically spend more time and cost later on rework and compliance remediation.
Can a custom healthcare CRM integrate with Epic?
Yes. Epic exposes a production-grade FHIR R4 API with SMART on FHIR authorization. Integration requires App Orchard registration and review (typically 4-8 weeks), a signed BAA with Epic, and FHIR R4 client development targeting the specific resource types required for the CRM’s use cases. Epic’s FHIR subscription API enables real-time sync for Encounter and patient status events, which is the mechanism that keeps CRM patient profiles clinically current.
What makes a healthcare CRM HIPAA-compliant?
HIPAA compliance in a CRM requires a signed BAA with the development vendor and all cloud infrastructure providers; AES-256 encryption at rest and TLS 1.2+ in transit for all PHI; role-based access control with minimum necessary access enforcement; immutable audit logs covering all PHI access events retained for six years; breach notification monitoring and documented response procedures; and a secure Software Development Life Cycle (SDLC) with documented risk analysis under the HIPAA Security Rule. HIPAA compliance is an architecture requirement that must be designed in from the first sprint.
How does AI improve patient communications in a healthcare CRM?
AI improves patient communications in three primary ways: dynamic patient segmentation (continuously re-scoring patients by risk, reachability, and engagement likelihood based on live clinical data); personalized message generation (drafting contextually accurate outreach based on the patient’s specific conditions, care plan, and communication history); and agentic workflow orchestration (executing multi-step follow-up sequences autonomously, monitoring for response, and escalating to care coordinators based on clinical rules). The compound effect is fewer no-shows, higher care gap closure rates, reduced readmission risk, and lower administrative workload for patient access staff.
Build the Data Layer First
The most common failure mode in healthcare CRM projects is treating the data layer as an implementation detail rather than the system’s foundation. Off-the-shelf platforms become expensive integration projects when organizations discover that real-time FHIR sync, CCPA data segregation, and agentic AI orchestration require architecture the platforms were not designed to support.
Custom AI healthcare CRM development starts with the right questions: Which EHR systems require real-time sync? Which clinical events should trigger communications workflows? How does the schema separate PHI from non-PHI to satisfy CCPA deletion rights? What does human-in-the-loop oversight look like for AI-generated patient outreach? Getting the architecture right before writing application code determines whether the system performs in a clinical environment or becomes a compliance liability.
If you are evaluating a custom AI healthcare CRM build or planning an EHR integration architecture review, talk to a TATEEDA solution architect. We have worked with US health systems and digital health organizations on exactly these decisions since 2013 — and we sign the BAA before the first line of code is written.