Agentic AI in Healthcare 2026: Everything to Know, Trends and Types

Slava Khristich



Vlad Nazarov

Healthcare leaders are looking past demos to real deployment. In this guide you’ll get a clear view of healthcare AI agent trends in 2026: what is being built, how agentic AI is used in custom healthcare software development solutions today, where it pays off, typical costs and build options, and what to watch as multi-agent AI models for healthcare are taking over routine bureaucratic and research processes that once fell to clerks and administrative staff.
Healthcare is moving from AI that predicts or interprets (like AI for medical diagnostics) to AI that acts on behalf of human specialists. Instead of single-purpose models, agentic AI in healthcare introduces goal-driven “digital teammates” that perceive context, plan, choose tools, and execute steps across clinical and operational workflows. The shift is measurable: the FDA now lists 1,000+ AI/ML-enabled medical devices cleared for the U.S. market; industry trackers put the total above 1,200 by July 2025, and 2024 set a record with 235 authorizations. This is evidence that regulated, workflow-aware software is moving beyond static prediction.
What exactly is an AI agent in healthcare? Think of a system designed to pursue a defined objective within real workflows. It maintains short-term memory and context, maps multi-step plans, calls APIs and enterprise tools, and adapts when conditions change. Autonomy sits on a spectrum: assistive agents that structure clinician and patient conversations, collaborative agents that co-pilot care by suggesting actions and presenting evidence, and narrowly scoped autonomous agents that execute pre-approved tasks under strict guardrails. This is where we build custom healthcare AI agents that respect risk tiers and safety cases.
Momentum is visible in hospital operations: 71% of U.S. hospitals in 2024 reported predictive AI integrated with the EHR, up from 66% in 2023, a sign that data and workflow plumbing are ready for agents that act on events rather than only score risk. Ambient documentation shows similar traction: Kaiser Permanente logged 2.5 million uses and 15,000 hours saved in one year, and peer-reviewed evidence reports about 28.8% shorter documentation time per encounter among high-use clinicians, which frees attention for patients and creates a reliable audit trail.
Commercial platforms are also normalizing agent behavior. OpenAI’s Operator previewed agents that can navigate software, fill forms, and complete tasks end to end. This is an example of general-purpose capabilities that health systems can adapt with HIPAA-aligned controls.
Against this backdrop of healthcare AI agent trends, this article explains how agentic AI is used in healthcare, what it costs to build or buy, and how to measure ROI. We cover the building blocks (memory, planning, tool use), governance (human-in-the-loop, auditability, PHI-safe data flows), and practical architectures, including multi-agent AI models for healthcare that coordinate intake, patient communications, prior authorization, documentation, device monitoring, and revenue cycle, so you can design systems that are useful, interoperable, and trustworthy at scale.
Ready to Build AI Agents That Do the Work?
Build healthcare AI agents for documentation, patient messaging, prior auth, device alerts, and revenue cycle.
Why we’re qualified to cover agentic AI development trends and solutions
Since 2013, TATEEDA, as a San Diego custom software development solution provider, has designed, built, and operated HIPAA-grade clinical and operational systems for U.S. healthcare. Our teams work in real production environments, not labs, which is why we track healthcare AI agent trends in 2026 and apply agentic AI in healthcare where it actually works. We have shipped EHR-connected apps, revenue-cycle tooling, and workforce platforms at the national scale, so we understand how agentic AI is used in healthcare when uptime, privacy, and auditability matter.
We don’t just comment on the space; we build healthcare AI agents and multi-agent AI models for healthcare that run inside existing workflows. Below is how that experience translates into dependable delivery:
- Production immersion: We have mapped bottlenecks across credentialing, onboarding, scheduling, timekeeping, compliance reviews, and audit trails. Those lessons inform agent designs that remove real friction without breaking established routines.
- Agent system design: We architect multi-agent solutions with clear roles: a planner or orchestrator, tool-using specialists, and a verifier. Each step is explicit and auditable, so stakeholders can see what happened, why, and with which data.
- Governance you can trust: We implement least-privilege execution, role-based access, PHI minimization, consent and provenance tracking, and immutable logs with human approval gates. This aligns agent behavior with policy and clinical oversight.
- Integration depth: We connect to the backbone that agents depend on: FHIR R4 read and write, HL7 v2 feeds, SMART on FHIR launches, payer and clearinghouse APIs, device clouds, scheduling, secure messaging, and analytics pipelines. That is the substrate for orchestration across EHR and back-office systems.
- Verification first: We add deterministic checks for citations, data types, thresholds, payer edits, NCCI rules, and internal policies. When a check fails, the system replans the minimal step, which cuts rework and improves quality.
- Operate with confidence
We ship with acceptance tests, drift and quality monitors, canary releases, rollbacks, dashboards, and runbooks. Leaders can see the effect of agents in near real time and act on dependable signals. - Delivery model that scales: U.S. discovery and architecture combined with nearshore engineering for speed and value. This lets programs move from pilot to steady state without losing control or visibility.
Result: We are a practitioner-level dedicated software development company that understands large clinical and HR workflows and knows how to automate them with agentic AI in healthcare. If you want a partner who can speak clearly about healthcare AI agent trends, design the architecture, and ship production-ready systems, we’re set up to do exactly that.

Table of Contents
Market Trends for Agentic AI in Healthcare: 2025 Signals, 2026 Trajectory
Agentic AI is moving from interesting pilots to funded programs with production goals. Venture data shows momentum: U.S. digital-health startups raised $6.4B across 245 deals in H1 2025, and analysts note that AI-enabled companies captured a majority of that capital; their average round—$34.4M—was far larger than non-AI peers, a sign that investors want workflow automation rather than one-off chat tools.
On the delivery side, health systems began publishing early output metrics for agents living inside daily workflows: one example is Hackensack Meridian Health’s note-summarization agent, which supported 1,200+ clinicians and produced 17,000+ summaries within months of launch. Buyer signals are formalizing too: KLAS introduced its first Best in KLAS: Ambient Speech rankings and published a dedicated outcomes analysis, giving procurement teams benchmarks for this maturing agent category (2025 ranking; KLAS ambient report).
The runway into 2026 is shaped by two countervailing forces: budgets that are expanding for automation and organizations that still need foundational readiness. A HIMSS Market Insights study found only 18% of healthcare organizations consider themselves “AI-ready”, which explains strong demand for integration, governance, and change-management services (Healthcare IT News summary).
At the same time, industry forecasts expect a sharp acceleration in spending—IDC projects healthcare generative-AI investments will triple by 2026, shifting attention from chat to agents that plan, act, and verify across systems. Put together, the market picture is clear: money and early results are in place; the winners in 2026 will be teams that operationalize agents with solid data plumbing, oversight, and measurable outcomes.
2025–2026 Market Signals and Agentic AI Development Trends at a Glance
| Trend | Evidence (linked) | Why it matters in 2026 |
|---|---|---|
| Capital concentrates in AI | $6.4B across 245 deals in H1 2025; AI-enabled startups took the majority, with $34.4M average rounds (Rock Health overview; AI deal sizes) | Capital concentrates on AI |
| Real deployments report output | 1,200+ clinicians and 17,000+ summaries from one note-summarization agent in early rollout (Healthcare Dive; press release) | Proof that agents can live inside routine clinical documentation with measurable throughput. |
| Category maturation | Best in KLAS: Ambient Speech 2025 rankings and outcomes research (ranking; report) | Buyers get benchmarks for performance, integration, and satisfaction—accelerating enterprise adoption. |
| Readiness gap | Only 18% of orgs say they are AI-ready (HIMSS study summary) | Drives demand for integration, data governance, and change-management work around agents. |
| Spend outlook | GenAI investments will triple by 2026 in healthcare (IDC predictions) | Budgets expand for agentic AI that achieves end-to-end outcomes with safety and oversight. |
Bottom line: the market is primed. Investment is flowing to agentic platforms, early production numbers are public, and independent benchmarks now exist. The next leg of growth arrives in 2026 as organizations scale from conversational pilots to agents that reliably move work to “done.”
AI Agents vs. Traditional Conversational AI in Healthcare: What Changes in 2026
In 2026, one of the most notable healthcare AI agent trends is a shift from single-turn chat to agentic AI in healthcare, which plans, acts, and verifies across real-world workflows. Instead of answering questions, agents execute steps, call tools, and write back to EHRs with audit trails. This comparison illustrates how the direction trends in AI agent development are heading and how current technologies in AI agent development for healthcare impact scope, safety, and outcomes.

| 🧠📋 How to read this: if the job is “answer a question,” conversational AI is fine. If the job is “move a task to done,” you need agents that can remember state, plan, call systems, and verify results. |
| Dimension | Traditional Conversational AI | Healthcare AI Agents (Agentic) |
|---|---|---|
| Primary goal | Respond to a query | Achieve an outcome across steps |
| Scope of work | Single task or answer | End-to-end workflow execution |
| Autonomy | Reactive; user-driven | Proactive; event- and goal-driven |
| Memory | Short session context | Short-term task memory; persistent state as needed |
| Planning | Minimal | Multi-step plans with replanning on feedback |
| Tool use | Limited lookups | Structured tool calls: EHR, payer, device, analytics APIs |
| Orchestration | One model, one turn | Audit trails, provenance, consent capture, and role-based access |
| Reasoning patterns | Prompting, few heuristics | Answer the benefits question |
| Verification | Ad hoc | Deterministic validations, policy rules, data-type checks |
| Governance | Basic logs | Prompting, a few heuristics |
| Interoperability | Links or simple queries | FHIR/HL7 read-write, workflow engines, reliable EHR write-backs |
| Human-in-the-loop | User confirms answers | Checkpoints for approvals; escalation paths |
| Reliability focus | Response quality | Task completion rate, error containment, safe fallback |
| Example use | Tool misuse, policy violation, caught by verifiers and guards | Complete prior auth packet; reschedule visit; draft and file note |
| Typical metrics | CSAT, deflection | Time saved, first-pass yield, denial rate, throughput |
| Failure modes | Irrelevant answers | Multi-step plans with replanning based on feedback |
| Build approach | Chat UX + FAQ knowledge | Event triggers + planning + tools + verification + monitoring |
| Scale path | More intents | More agents and tools; stronger routing and observability |
| Fit in 2026 | Useful for help and triage | Core engine for repeatable clinical and operational work |

How Agentic AI Works in Healthcare: Memory, Planning, and Tool Use That Drive Real Work
Core Building Blocks
Agentic systems for healthcare combine five cooperating blocks that turn intent into action inside real workflows:
- Perception: ingest signals from EHR events, documents, images, device streams, and chats.
- Short-Term Memory: retain task state and clinical context across steps.
- Planning: break a goal into steps, order them, and choose tools.
- Tool Execution: call APIs, databases, and apps, then write results back to operational systems.
- Feedback: validate outputs, learn from errors, and adjust the plan.
This architecture underpins many healthcare AI agent trends expected in 2026 because it creates agents that are inspectable and auditable rather than opaque.
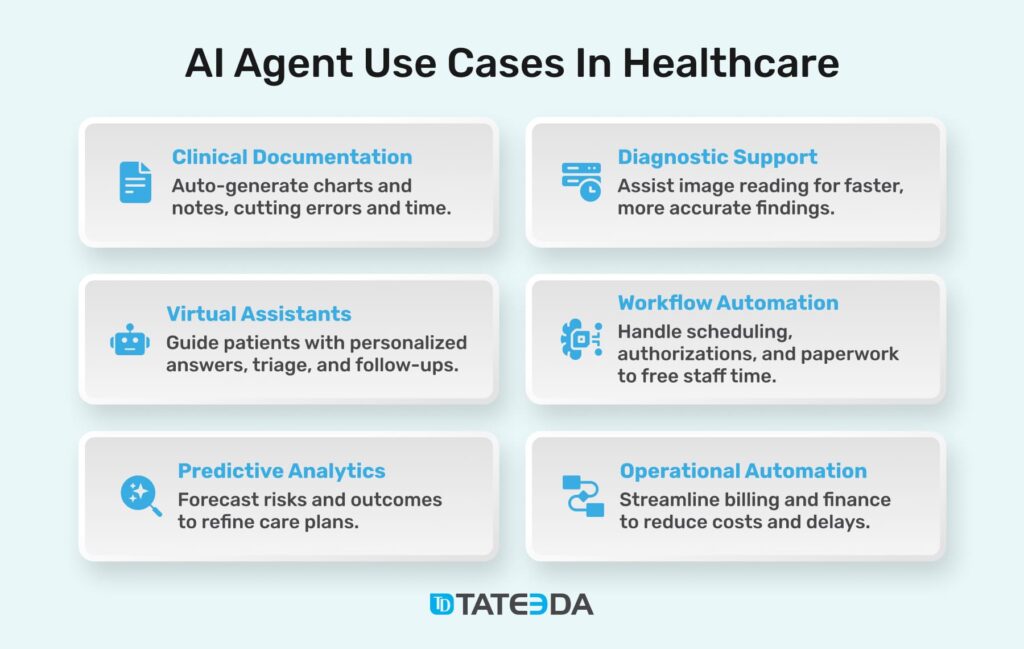
Agent Types in Demand for 2026
Signals from late 2025 show demand shifting from single chatbots to workflow agents that move work forward. Hospital leaders emphasized embedded, operational AI over demos in HIMSS 2025 takeaways, while Microsoft highlighted “copilot plus agent” patterns scaling across care teams at HLTH 2025, and Hackensack Meridian Health announced new agent pilots on Google Cloud in documentation and follow-up automation. Expect growth in:
- Ambient Documentation Agents: structure encounters, generate summaries, file notes with citations.
- Patient Communication and Scheduling Agents: guide intake, reminders, rescheduling across web, mobile, and phone.
- Prior-Authorization and Revenue-Cycle Agents: assemble packets, check policies, reconcile denials, and draft appeals.
- Remote Monitoring and Device Agents: triage physiologic signals, escalate alerts, coordinate outreach.
- Research and Quality Agents: retrieve literature, track measures, and prepare submission artifacts.
These examples reflect trends in AI agent development toward agents that execute end-to-end tasks inside existing systems.
Single-Agent vs. Multi-Agent Patterns
Both patterns matter when teams build healthcare AI agents:
- Single-Agent Designs: one planner with a tool used for narrow jobs, for example, assembling a prior-auth summary or drafting a discharge letter.
- Multi-Agent AI Models for Healthcare: roles improve reliability and separation of duties:
- Planner/Orchestrator (PEV: Planner): decomposes work and routes tasks.
- Tool Specialists (PEV: Executor): call EHR, payer, device, or analytics APIs.
- Verifier (PEV: Verifier): checks outputs against policies, thresholds, and data types.
Modern stacks ship these patterns so up-to-date technologies in AI agent development for healthcare are within reach: Google’s Vertex AI Agent Builder supports multi-agent orchestration and connectors, and Microsoft’s Azure AI Agent Service demonstrates administrative and research workflows.
Reasoning Strategies You Will See in Production
Teams increasingly combine lightweight reasoning methods to boost task completion and auditability:
- ReAct: interleave reasoning with tool calls; useful for stepwise prior-auth checks.
- Tree of Thoughts: explore alternatives before selecting a plan for complex clinical admin flows.
- PEV AI Agents: explicit Planner–Executor–Verifier separation with deterministic verification.
Agentic patterns are also normalizing in general software delivery. Microsoft reported 15 million developers using GitHub Copilot and introduced agent modes for planning, code review, and troubleshooting in its Build 2025 keynote, which accelerates enterprise adoption of agent workflows.
Data Plumbing and Governance That Make Agents Real
Interoperability advances reduce brittle integrations and enable auditable write-backs:
- Nationwide Exchange: Epic reported more than 1,000 hospitals and 22,000 clinics connected to TEFCA via Epic Nexus.
- QHIN Backbone: the Designated QHINs directory continues to expand, giving agents a national exchange network to rely on.
- FHIR Momentum: global use of FHIR rose in 2025, supplying structured access for safe EHR read and write operations; see Firely’s 2025 analysis and the HL7/Firely survey report.
For clinical and revenue workflows, effective agents run with human-in-the-loop checkpoints, audit trails, PHI-safe data flows, consent and provenance tracking, and clear escalation paths. Common patterns include event-driven triggers, workflow engines for long-running jobs, and EHR write-backs that record citations and reasons. This aligns with where healthcare AI agent trends are heading in 2026: dependable, policy-aware action at scale.
Major Trends in Agentic AI for Healthcare Support
Agentic AI is gaining traction because the digital plumbing is finally in place. Nearly all U.S. hospitals (≈96%) now use certified EHRs, giving agents a reliable substrate for context, tool calls, and write-backs. Patient interactions are also shifting online; telehealth use rose 6.13% from July to December 2024, which adds more digital touchpoints that agents can act on, from intake to follow-ups (FAIR Health telehealth tracker). With this infrastructure, healthcare AI agent trends point to task automation that runs inside existing systems rather than standalone chat.
The economics favor agents as well. U.S. health spending reached $4.9 trillion in 2023 (17.6% of GDP), keeping pressure on leaders to reduce administrative load and speed throughput. There is clear headroom: the 2024 CAQH Index estimates a $20B savings opportunity from automating routine transactions such as eligibility, claims, and prior authorization. Burden signals remain high; an AMA survey in 2025 found clinicians complete about 39 prior authorizations per week and spend ~13 hours on the process, with most reporting burnout contributions. These numbers explain why agents that plan, execute, and verify across support workflows are set to expand in 2026.
Where agents fit today: the table summarizes common support domains and the tasks that benefit most from agentic automation.
| Patient Onboarding and Engagement | Virtual Care Assistants | Clinical Record Management | Operational Workflow Automation | Revenue Cycle Management |
|---|---|---|---|---|
| Medical-history intake | Symptom checking | Conversation capture | Discharge planning | Insurance eligibility checks |
| Insurance verification | Aftercare guidance | Key-detail extraction | Resource scheduling | Code validation and edits |
| Personalized reminders | Care-team coordination | EHR auto-population | Delay detection and escalation | Claim generation and attachment prep |
| Language support and instructions | Medication-adherence nudges | Clinical coding assistance | Bed and room management | Denial prediction and appeals prep |

Takeaway: with near-universal EHR adoption, steady telehealth growth, and measurable admin pain points, 2026 is primed for agentic AI that works inside real workflows: planning steps, calling tools, verifying outputs, and leaving an audit trail.
Where Agentic AI Pays Off: Costs, Build Paths, and the Multi-Agent Shift
Agentic AI earns its keep where work is repetitive, policy-bound, and spread across systems. Think intake and patient communications, ambient documentation, prior authorization packets, revenue cycle follow-ups, device alerts, and research admin.
This is how agentic AI is used in healthcare today: agents hold short-term memory, plan steps, call tools, and verify outputs. As multi-agent AI models for healthcare mature, they are replacing the clerical grind with planner–executor–verifier loops that finish tasks and leave an audit trail.
Where It Pays Off Now:
- Ambient documentation: auto-draft notes with citations; reviewers accept or edit.
- Prior authorization: collect criteria, attach evidence, submit, track status.
- Patient communications: confirmations, reminders, rescheduling, post-visit guidance.
- Revenue cycle helpers: code suggestions, denial prediction, appeal drafts.
- Research ops: literature pulls, protocol checklists, dataset assembly.
| Use case | Success signals and time to impact |
|---|---|
| Documentation copilot | Measures include minutes saved per encounter, reduction in after-hours EHR time, percentage of notes finalized the same day, acceptance rate of AI-drafted summaries without edits, and clinician satisfaction scores. Secondary indicators include fewer copy-paste errors, clearer attribution of sources in the chart, and consistent use of required templates. Most teams see visible gains after a short tuning period, typically within 2–6 weeks once specialty prompts, citation formats, and review workflows are in place. |
| Prior authorization agent | Track first-pass approval rate, total turnaround from order entry to decision, manual touches per case, and the share of submissions that include complete evidence on the first attempt. Additional indicators include fewer payer reworks, cleaner audit trails for criteria used, and faster clinician sign-off on packet contents. Results generally materialize in 6–10 weeks after payer rules, medical policies, and document checklists are encoded and tested across a representative set of services. |
| Patient communications agent | Key metrics are no-show reduction, percentage of self-service confirmations and reschedules, median response time to inbound questions, and call-center deflection to secure messaging. Supporting signals include smaller message backlogs, higher portal engagement, and improved survey scores for clarity and timeliness. Most organizations observe impact within 4–8 weeks once the agent is connected to scheduling, reminders, and preferred patient channels with opt-in and consent captured. |
| Revenue cycle agent | Monitor initial claim acceptance rate, denial composition by reason, days in A/R, appeal turnaround, and cost to collect. Look for a higher proportion of touchless clean claims, fewer coding discrepancies flagged downstream, and better documentation to support medical necessity. Meaningful movement typically appears in 8–12 weeks after payer edits, code libraries, and appeal templates are integrated with billing systems and work queues. |
| Research admin agent | Success shows up as faster creation of literature packets, fewer revision cycles on protocol checklists, improved completeness of IRB submissions, and shorter lead times for grant or registry packages. Secondary gains include traceable citations, standardized document structures, and clearer task handoffs for reviewers. With domain prompts and reference sources curated, most teams record improvements within 4–10 weeks. |
Build Paths With Ballpark Cost and Time
These figures are for information only. Real effort depends on scope, data flows, integrations, risk controls, and team makeup. For a precise plan, speak with custom software development specialists at TATEEDA; we can review your requirements and provide a free estimate.
- Buy (best for narrow or ambient use cases): quickest path to value; still needs integration, access controls, and monitoring.
- Treat integration like a small pilot: 2–3 engineers + QA + PM, 8–12 weeks, $120k–$300k.
- Build (strong control for regulated or cross-system work): custom agents inside your stack with full policy and data ownership.
- Typical department rollout with EHR, payer, and messaging integrations: 5–8 engineers + QA + PM + architect, 3–6 months, $400k–$1.2M.
- Hybrid (vendor core plus custom agents): common choice for hospitals and payers needing flexibility and scale.
- Enterprise multi-agent program with planner, tool specialists, verifier, and monitoring: 8–15 engineers + QA + PM + architect + DevOps, 6–12 months, $1.2M–$3M.
- Operating costs (all paths): model and retrieval calls, observability, policy checks, and support; plan $8k–$50k per month depending on volume and model selection.
Final Word: Get Your Custom Agentic AI Solutions Designed and Delivered
Agentic AI in healthcare is no longer a demo; it is a work engine. The strongest healthcare AI agent trends point to systems that plan tasks, call tools, verify results, and leave an audit trail. That is how agentic AI is used in healthcare today: intake and patient communications, ambient documentation, prior authorization packets, device alerts, and revenue cycle handoffs. The next step for 2026 is scale: organizations will build healthcare AI agents that operate inside EHRs and payer stacks, often as multi-agent AI models for healthcare with clear roles such as planner, tool specialist, and verifier.
TATEEDA helps you get there without guesswork. We are a dedicated software development company with senior engineers who connect FHIR and HL7, payer and clearinghouse APIs, device clouds, and analytics pipelines. Our teams design agents with short-term memory, planning, and tool use, then add human-in-the-loop checkpoints, PHI-safe data flows, consent and provenance tracking, and deterministic validation. We document decisions as ADRs, ship through CI/CD, and monitor task completion, first-pass yield, and denial rates so ROI is visible.
Ready to move beyond chatbots? We scope use cases, model the workflow, and ship production-ready agents that fit your environment. If you want a partner who can read the market and build to it, TATEEDA is ready to help.