Multi-Agent AI in Healthcare: Practical Patterns, EHR/Payer Integrations, Results

Slava Khristich



Vlad Nazarov

This article offers a practical explanation of multi-agent AI systems in healthcare, showing how they connect to EHR and payer rails and why the approach is gaining momentum now, with an emphasis on patterns teams can actually use, the standards that make integration safe, and outcomes U.S. providers and HealthTech groups can measure.
In plain terms, a multi-agent system is a coordinated team of small, task-focused AI agents (custom AI-directed workflow bots) that share context and divide work across planning, data retrieval, drafting, and final checks; the flow usually moves from an initial decomposition of a vague request into auditable steps, to targeted execution through approved tools and APIs with least-privilege access and logging, and finally to verification against rules and data so the output is corrected or confirmed before it reaches a patient record or a payer system.
Scale is the first reason this matters: Medicare Advantage processed nearly 50 million requests for prior authorization in 2023, and 6.4% were denied, so even modest gains in how evidence is assembled and how criteria are checked can improve turnaround times for millions of decisions and reduce avoidable back-and-forth.
Policy is the second driver because buyers are being asked to prefer systems that can explain themselves; the ONC’s HTI-1 DSI criteria require certified health IT to expose source attributes and model facts, and the key dates starting in 2025 reinforce the expectation that decision support will be transparent, which aligns naturally with multi-agent designs that keep provenance and verifier logs by default.
Tooling has also matured beyond proofs of concept; the 2025 Ambient Speech rankings highlight strong satisfaction with production documentation assistants, and the same orchestration ideas extend from notes into triage, prior authorization, and revenue cycle tasks where agents gather inputs, call the right services, and return artifacts that are easy to audit.
The budget picture points the same way, with the PwC AI Agent Survey reporting 88% of U.S. executives plan to increase AI spending and 79% already adopt agents, which in healthcare intersects with FHIR and HL7, payer APIs, and compliance obligations, making multi-agent systems a practical way to scale trustworthy automation without introducing black-box behavior.
Taken together, teams choose multi-agent frameworks over a single chatbot because they turn disorganized multi-system work into traceable steps, integrate cleanly with FHIR R4, HL7 v2, SMART on FHIR, and payer EDI, and produce results that clinicians and finance leaders can review and approve before anything is written back.
Need immediate help with creating a multi-agent AI system?
Our engineers design, build, and govern agentic healthcare solutions with orchestrators, task bots, and a verifier layer for safety.
Why TATEEDA is qualified to talk about multi-agent AI solutions
Since 2013, TATEEDA, a custom software solution development company in San Diego (CA), has delivered HIPAA-grade healthcare systems for U.S. organizations and supported them in production. Our work with AYA Healthcare immersed us in large-scale clinical and HR workflows under real load, which now informs how we design multi-agent AI in healthcare that is dependable in day-to-day operations.
We mapped the bottlenecks in credentialing, onboarding, scheduling, timekeeping, compliance reviews, and audit trails—and we use those lessons to architect agentic AI for healthcare with coordinated roles (decomposer/orchestrator, tool specialists, and verifier) instead of a single opaque model.
We bring that experience to multi-agent development services focused on measurable outcomes and governance. The goal is straightforward: break work into auditable steps, route each step to the right tool or agent, verify against rules and data, and hand off with evidence your teams can trust.
- Agents built for real work: clinical documentation copilots, triage and intake flows, prior-auth packet builders, RPM signal filters, revenue-cycle helpers. From AYA, we also carry recruiters and staff copilots, credential checks, schedule optimization, and timesheet validation.
- Governance you can audit: least-privilege execution, role-based access, PHI minimization, consent and provenance tracking, immutable logs, and human approval gates.
- Integration depth: FHIR R4 read/write, HL7 v2 feeds, SMART on FHIR launches, payer and clearinghouse APIs, device clouds, scheduling, and secure messaging—the backbone for multi-agent orchestration across EHR and back-office systems.
- Verification first: deterministic checks for citations, data types, thresholds, payer edits, NCCI rules, and policy constraints. Failures trigger targeted re-plans, reducing rework and elevating quality.
- Operate with confidence: acceptance tests, drift and quality monitors, canary releases, rollbacks, dashboards, and runbooks so leaders can see impact and act on it.
- Nearshore delivery that scales: U.S. discovery and architecture with nearshore engineering in LATAM and Europe for speed, overlap, and value—our model for multi-agent programs from pilot to steady state.
Result: a partner that understands large healthcare and HR workflows from hands-on delivery, and knows how to automate them with multi-agent systems that are auditable, reliable, and production-ready.

Table of Contents
Core Multi-Agent AI System Architecture: Orchestrators, Specialists, and the Observer
In a multi-agent AI architecture, three roles keep everything understandable and safe, and they refer to separate software components that work together to produce a verified result. The orchestrator breaks a request into smaller steps, assigns those steps to focused specialist agents, and keeps a running memory of what happened. The observer (often called the verifier) checks every important output against rules, data, and policy before anything reaches the EHR or a payer system. Think of it as multi-agent orchestration that plans, acts with tools and APIs, then proves the result is correct.
Terminology used in multi-agent AI solutions:
- Orchestrator: a coordinator who turns a vague goal into a step-by-step plan and routes work.
- Specialist agent: a task bot that does one job well, like reading FHIR, packaging a claim, or summarizing a note.
- Observer/verifier: an assurance layer that validates fields, thresholds, citations, and compliance signals.
- Shared memory/blackboard: the place where agents post inputs, outputs, and decisions so the team stays in sync.
- Message passing: structured messages that move plans, results, and errors between roles without ambiguity.
Engineering habits that make multiagent systems (MAS) dependable:
- Contracts for inputs and outputs, defined as JSON schemas and tested in CI
- Idempotent writes to EHR and payer rails, with retries and exponential backoff for flaky endpoints
- Least-privilege identities and scoped access, with full provenance on every write
- Deterministic verification rules, so “pass” and “fail” mean the same thing every run
“Multi-agent systems earn trust when they show their work. Plans are explicit, tools are well-scoped, and every result includes proof you can trace,”
— Slava K., TATEEDA CEO.
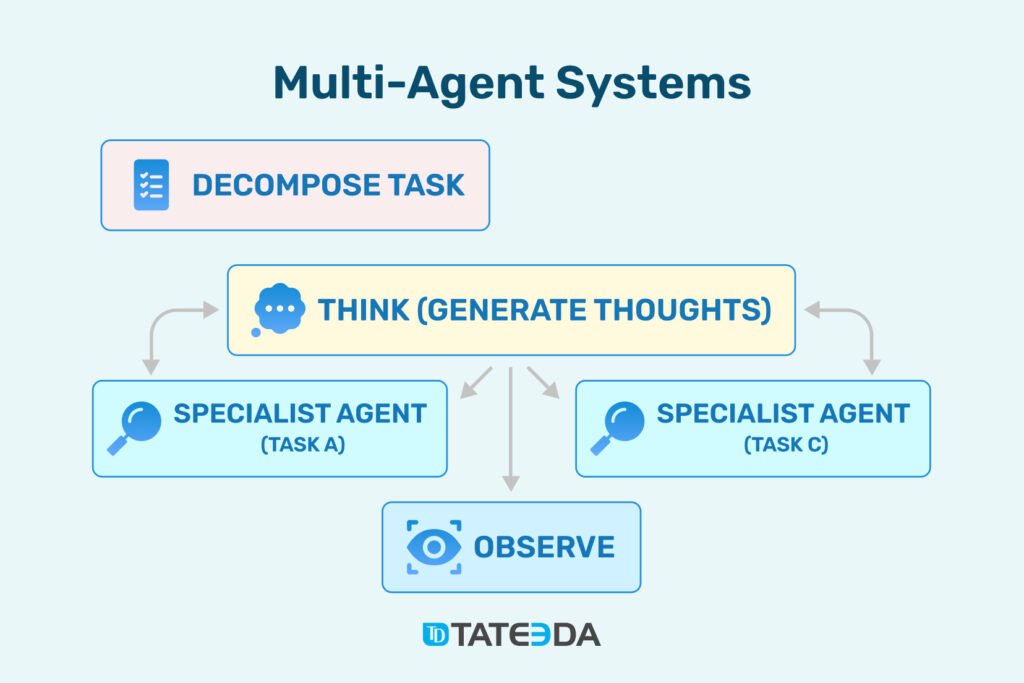
This diagram illustrates multi-agent development: a Decomposer splits a clinical task, a Think/Coordinator plans actions, specialist agents execute focused steps, and an Observer checks results for accuracy and safety. In multi-agent AI in healthcare, this multi-agent orchestration lets a MAS pull EHR data, assemble prior-authorization packets, draft notes, and verify outputs before anything is written back or submitted.
Where multi-agent AI cascades show up in healthcare practice:
- Clinical documentation assistant: the orchestrator outlines SOAP sections, a specialist transcribes and drafts, another pulls meds and allergies via FHIR, and the observer checks required fields and contradictions before a draft lands in the chart. This is practical multi-agent AI in healthcare, not a black-box chatbot.
- Prior authorization: the orchestrator maps payer criteria, a data agent fetches labs and imaging, a packaging agent builds a 278 or payer FHIR packet, and the observer rejects submissions missing attachments. Clean packets shorten cycle times.
- Revenue cycle and claims: a coding agent proposes ICD and CPT, a rules agent enforces NCCI edits, and the observer blocks any bundle that fails payer checks. This pattern pairs well with custom patient billing software development when you aim to achieve first-pass yield improvements.
- Remote patient monitoring: a signal agent normalizes device data, a baseline agent detects outliers, and the observer cross-checks against medication lists and protocols. Only actionable alerts reach clinicians.
- Clinical trials and pharma workflows: a matcher agent screens inclusion and exclusion, a literature agent attaches evidence, and the observer verifies protocol alignment before notifying staff. Teams often fold this into custom pharmaceutical software development to streamline study operations.
When leaders ask why agentic AI for healthcare is gaining ground, the answer is simple. Multi-agent frameworks carve complex, multi-system work into verifiable steps. They plug into EHR and payer standards without overreach. They leave a trail that compliance can audit and operations can trust. And because each agent does one job with clear contracts, you can grow coverage safely, one proven workflow at a time.
Methods Used to Build Multi-Agent Systems
Effective multi-agent development begins with a step graph. Instead of a single prompt that tries to do everything, you define a sequence of small moves that a coordinator can schedule and a set of outcomes each move must produce. The graph doubles as documentation and as a control surface, since you can pause a branch, retry a node, or swap in a different specialist without touching the rest of the flow. In multi-agent AI in healthcare, common step graphs cover intake, evidence gathering, drafting, packaging, and finalization, each tied to concrete success signals.
Prompt schemas keep planning stable. Give the orchestrator a compact schema for the plan it should produce and require specialists to read and write the same schema shapes. This keeps multi-agent orchestration predictable even as you add new skills. When specialists call tools, they do it through adapters that hide system quirks and return typed outputs: FHIR reads and writes for the EHR, retrieval for knowledge, parsers for documents, schedulers for time slots, and device-cloud adapters for streams from home monitoring.
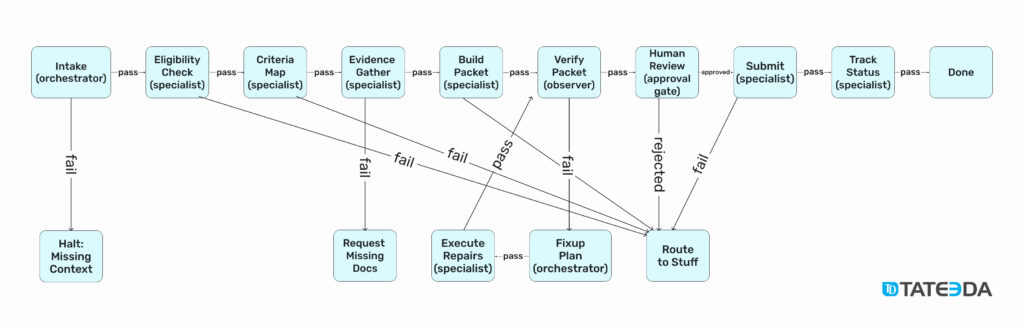
This diagram is a compact example of multi-agent system design for prior authorization in healthcare.
| 📋✅ Prior authorization (PA) is a cost and quality control step used by health insurers. Before certain tests, procedures, medications, or equipment are covered, the insurer asks the provider to submit clinical evidence that the service is medically necessary under the patient’s plan. |
It shows multi-agent orchestration as a step graph: the orchestrator normalizes context in Intake, then routes work through specialist agents for Eligibility Check, Criteria Map, Evidence Gather, and Build Packet. An observer in Verify Packet runs executable checks against payer rules and data, and if anything fails the flow drops into a small Fixup Plan and Execute Repairs loop rather than restarting the entire process.
A human approval gate appears before Submit so a clinician or revenue-cycle lead can review the assembled packet with evidence. Idempotent Submit captures a tracking ID, and Track Status closes the loop. Pass and fail edges make the control flow explicit, retries happen within nodes, and every transition leaves a trace in shared memory. The legend to remember is simple: plan as small steps, delegate to focused agents with tool adapters, verify with deterministic rules, and surface clear checkpoints where people approve high-impact actions.
Verification must be executable, not narrative. Write rules that can run automatically and return pass or fail with reasons, then gate downstream actions on those results. Attach human approval where risk is high, such as committing diagnoses, signing orders, or submitting sensitive payer transactions. Slava K., TATEEDA’s CEO, puts it plainly:
“Multi-agent systems succeed when every step is small, every tool call is scoped, and every result carries proof that a clinician or auditor can quickly understand.”
To make multiagent systems (MAS) durable, version each adapter, track acceptance rates by step, and record provenance with the output so later reviews are routine rather than forensic. Start with one end-to-end slice and grow coverage by cloning patterns, not by inventing new ones for every service line. That is how agentic AI for healthcare moves from concept to daily use.
| Method area | What it is | Practical tip | Example in healthcare |
|---|---|---|---|
| Step graphs | Ordered nodes with clear outcomes | Pause and retry nodes independently | Intake → evidence → draft → finalize |
| Prompt schemas | Compact JSON for plans and results | Keep fields stable as you add skills | Plan sections for a SOAP draft |
| Tool adapters | Safe wrappers for systems | Return typed outputs only | FHIR reads, document OCR, scheduler API |
| Verification checks | Executable rules with reasons | Gate high-risk actions on pass | Prior-auth criteria and attachment checks |
| Human approval | Explicit review points | Show evidence with each request | Clinician sign-off before chart writeback |

What You Can Automate Right Now with Multi-Agent AI in Healthcare
Think of multi-agent AI in healthcare as a small team of digital coworkers that handle the repeatable steps your staff does every day, while your clinicians and revenue leaders keep the final say. An orchestrator plans the flow, specialist agents fetch data and perform discrete actions through approved APIs, and a verifier blocks anything incomplete or inconsistent before it reaches the EHR or a payer system. This is multi-agent orchestration in practice: clear roles, short steps, and visible proof of how each result was produced.
“Multi-agent systems earn trust when they show their work. Plans are explicit, tools are well-scoped, and every result includes proof you can trace,” — Slava K., TATEEDA CEO.
Use the table below as a quick map rather than a deep dive. Each row outlines a common workflow, the concrete jobs the agents perform, and the systems they touch—including custom EHR/EMR software development solutions—so decision-makers can see where a pilot would land and which teams need to be involved.
Pick one area where the pain is already measured—documentation time, pend rates, first-pass yield, no-show rates, or alert burden—then start small, confirm the gain, and expand your multiagent systems (MAS) coverage only when the numbers hold.
| Workflow | What the multi-agent system does (step-by-step) | Key data and systems it uses | Practical outcome |
|---|---|---|---|
| Clinical notes | Draft → check → sign: an intake agent turns visit audio into text, a chart agent pulls meds, allergies, and vitals, a drafting agent creates a SOAP note, and a verifier flags missing fields or contradictions before clinician sign-off. | EHR via FHIR R4 (MedicationStatement, AllergyIntolerance, Observation), speech-to-text, terminology services (ICD-10-CM, SNOMED CT), provider inbox for approval. | Less after-hours charting and more consistent note quality. |
| Prior authorization | Gather → package → submit: an eligibility agent checks coverage, a criteria agent maps the ordered CPT/HCPCS to payer policy, an evidence agent fetches notes, imaging, and labs, a packet agent fills the request, and a verifier checks completeness and code alignment before submission and tracking. | EDI 270/271 or payer FHIR Coverage for eligibility, EHR documents (H&P, progress notes), PACS reports, lab results, request via EDI 278 or payer PriorAuth FHIR, status via 276/277. | Fewer pend letters and faster determinations. |
| Billing / coding | Propose → validate → file: an NLP agent extracts diagnoses and procedures from notes, a coding agent proposes ICD-10-CM and CPT/HCPCS, a verifier runs NCCI edits and payer rules, then a claims agent builds the file and monitors status. | EHR notes and op reports, coding references (AMA CPT, CMS NCCI), clearinghouse APIs, 837P/837I claim files, remittance via 835. | Cleaner first-pass claims and fewer rework cycles. |
| Intake / scheduling | Collect → triage → book: an intake agent asks adaptive questions and pre-fills forms, an eligibility agent verifies benefits, a scheduler holds the right slot, and a reminders agent confirms attendance; a verifier ensures consents and forms are complete. | Patient portal, ID capture and OCR, EDI 270/271 benefits check, EHR scheduling API, messaging (SMS/email), e-consent repository. | Higher show rates and less front-desk back-and-forth. |
| Remote Patient Monitoring (RPM) | Filter → assess → escalate: a device agent ingests wearable/at-home readings, a baseline agent compares to personal thresholds, a verifier cross-checks meds and diagnoses, and an alerting agent opens a task or messages the patient when action is warranted. | Device clouds (e.g., Dexcom, iRhythm, Apple HealthKit, Google Fit), EHR FHIR Observations, medication/problem lists, secure messaging or tasking system. | Fewer false alarms and timelier interventions. |
How to read this: each row shows a small team of agents working together—the orchestrator plans the steps, specialist agents call the right systems, and an observer/verifier blocks anything that isn’t complete or consistent before it touches the record or a payer portal.
How Multi-Agent Systems Fit Your Existing EHR and Payer Setup
You don’t need a new EHR or a risky rebuild. Think of multi-agent AI in healthcare as a sidecar that uses the standards you already have, then adds coordination, shared memory, and a final safety check. Agents read and write through approved APIs with narrow permissions, and every action is logged so you can see what happened and why.
Most organizations rely on three simple “roads.” First, EHR data through FHIR R4 lets agents read meds, allergies, problems, and vitals, and save drafts for human review. Second, HL7 v2 event feeds tell agents when an order, admission, or result arrives so they can start the right steps immediately. Third, payer connections through EDI and newer payer FHIR endpoints handle eligibility, prior authorization, claim status, and remittance.
What IT usually turns on:
- Credentials with narrow scopes, such as SMART on FHIR or backend service tokens.
- Network paths or gateways for the EHR, document stores, scheduling, and payer endpoints.
- Centralized logs so security and compliance can trace every run.
Fit map:
| Need | Standard path | Agent behavior |
|---|---|---|
| Pull chart context | FHIR read | Gather meds, allergies, problems, vitals for a safe draft |
| React to triggers | HL7 v2 events | Start a plan the moment an order or admit arrives |
| Submit to payers | EDI or payer FHIR | Build, verify, and submit clean payloads with evidence |
| Track outcomes | Status APIs | Poll decisions, record provenance, and notify staff |
Because each agent is a small, focused component, you can introduce one capability at a time, prove value, and expand without disrupting clinical flow. If you need deeper tailoring on the payer side, custom medical insurance software development can wrap these same standards with the exact benefit checks, prior-auth rules, and claims workflows your teams already use—while multi-agent orchestration keeps every step auditable and under your control.

Final Word: Get Multi-Agent Solutions Built for Your Medical Practice
If you’re ready to move from talk to results, we can help you design and ship multi-agent AI in healthcare that actually lightens the load. This article showed how multi-agent orchestration breaks work into small, verifiable steps, fits your existing EHR and payer rails, and protects safety with clear approvals and audit trails. We also walked through where to start—clinical notes, prior authorization, billing and coding, intake and scheduling, and remote patient monitoring—and what to measure so you can prove value before you scale.
What TATEEDA brings to your program:
- Architecture and build: orchestrators, specialist agents, and an observer layer with executable checks and human approval gates.
- Integrations that last: FHIR R4 reads and writes, HL7 v2 event listeners, and payer connections through EDI and payer FHIR for eligibility, prior auth, claim status, and remits.
- Governance by design: least-privilege access, consent and provenance, versioned adapters, drift and quality monitors, dashboards your leaders can read in minutes.
- Delivery you can trust: U.S. discovery and architecture with nearshore software engineering for speed, overlap, and sensible cost.
Our approach is simple. Pick one workflow with clear pain and baseline metrics. Stand up an end-to-end agent path that plans the work, calls the right tools, verifies the result, and pauses for a human when risk is high. Prove the gain. Then extend the pattern to the next process without disrupting clinical flow.
If you want multi-agent solutions that are auditable, reliable, and ready for daily use, TATEEDA is ready to partner with you—from the first pilot to steady-state operations.






