Planner–Executor–Verifier (PEV) Agents in Healthcare: A Practical Guide for U.S. Providers and HealthTech Teams

Andrii Morchenko

Vlad Nazarov

This article explains Planner–Executor–Verifier (PEV) agents in healthcare and shows where they deliver value fast. You’ll see how a Planner → Executor → Verifier (plus Critique) loop turns messy, multi-tool work into auditable steps, where agentic AI fits across clinical and operational workflows, which early outcomes signal real productivity gains, and a practical path from pilot to scale for PEV AI agent development services.
U.S. care delivery carries a heavy administrative load. The CAQH 2024 report identifies $20B in potential savings from moving manual tasks to electronic and automated transactions, and places routine administrative work near $90B annually. This is prime territory for PEV flows that plan steps, execute with tools, and verify before handoff.
Need immediate help with creating a custom PEV agent?
Our experienced engineers can advise you on designing, building, and governing Planner–Executor–Verifier (PEV) AI agents for healthcare.
Policy is accelerating the adoption of interoperable, verifiable workflows. Under the CMS final rule on Interoperability and Prior Authorization, impacted payers must meet key provisions by January 1, 2026, with API requirements beginning January 1, 2027. That timeline favors verify-before-submit patterns for prior authorization and FHIR-based APIs.
Clinical programs show measurable gains when systems plan the note, execute drafting, and verify against chart data before sign-off. At Northwestern Medicine, DAX Copilot users reported 24% less time on notes, 17% less after-hours “pajama time,” and capacity for 11.3 additional patients per month, which reflects a PEV-like loop that boosts throughput.
Adoption is scaling across large systems and adjacent industries. AMA report coverage cites 2.5 million uses and 15,000 hours saved in one year at The Permanente Medical Group. In life sciences, the McKinsey report estimates $60–$110B in annual potential value from generative AI across pharma and medical products, which supports demand for auditable PEV agents that orchestrate multi-step tasks with checks.
Why TATEEDA is qualified to talk about AI agent solutions
Since 2013, TATEEDA, a custom software solution development company in San Diego (CA), has delivered HIPAA-grade healthcare systems for U.S. organizations and supported them in production. Our work with AYA Healthcare exposed us to large-scale clinical and HR workflows in a real-world setting.
We learned the bottlenecks in automated medical staff credentialing, onboarding, scheduling, timekeeping, compliance reviews, and audit trails. Those lessons now guide how we automate these processes and how we design Planner–Executor–Verifier (PEV) agents in healthcare that are safe to run in production.
We bring that experience to PEV AI agent development services focused on measurable outcomes and governance. The goal is simple: plan the work, execute with the right tools and APIs, verify against rules and data, then hand off with clear evidence.
- Agents built for real work: Clinical documentation copilots, triage and intake flows, prior-auth packet builders, RPM signal checks, revenue cycle helpers. From AYA, we also bring recruiters and staff copilots, credential checks, schedule optimization, and timesheet validation.
- Governance you can audit: Least-privilege execution, role-based access, PHI minimization, consent and provenance tracking, immutable logs, and human approval gates.
- Integration depth: FHIR R4 read and write, HL7 v2 feeds, SMART on FHIR launches, payer and clearinghouse APIs, device clouds, scheduling, and secure messaging. This is the backbone for PEV healthcare AI assistants for EHR integration and back-office automation.
- Verification first: Verifiers check citations, data types, thresholds, payer edits, NCCI rules, and policy constraints. If a check fails, the agent re-plans or re-executes, which reduces rework and improves quality.
- Operate with confidence: We add acceptance tests, drift and quality monitors, canary releases, rollbacks, dashboards, and runbooks so teams can see the impact and act on it.
- Nearshore delivery that scales: U.S. discovery and architecture with nearshore engineering in LATAM and Europe for speed, overlap, and value. This is our model for nearshore AI agent development from pilot to steady state.
Result: a partner that understands large healthcare and HR workflows from hands-on delivery, and knows how to automate them with PEV agents that are auditable, reliable, and ready for production use.

Table of Contents
How PEV Works End to End in Healthcare Workflows
🕵️♂️🤔 First, what is an agent? In this context, an agent is a purpose-built AI program that accepts a goal, plans the necessary steps, and executes those steps using tools and APIs. Agents and other AI components can be integrated into an existing legacy product, such as a SMART on FHIR app in an EHR, or run as a sidecar service that connects multiple systems into a single automated workflow.
As demonstrated in the diagram, Planner–Executor–Verifier (PEV) agents in custom healthcare software development practices follow a tight loop. The Planner turns intent and clinical context into a step list with clear inputs and outputs. The Executor carries out those steps through adapters for FHIR, HL7 v2, payer, and clearinghouse APIs, schedulers, and storage, using least-privilege credentials with full tracing.
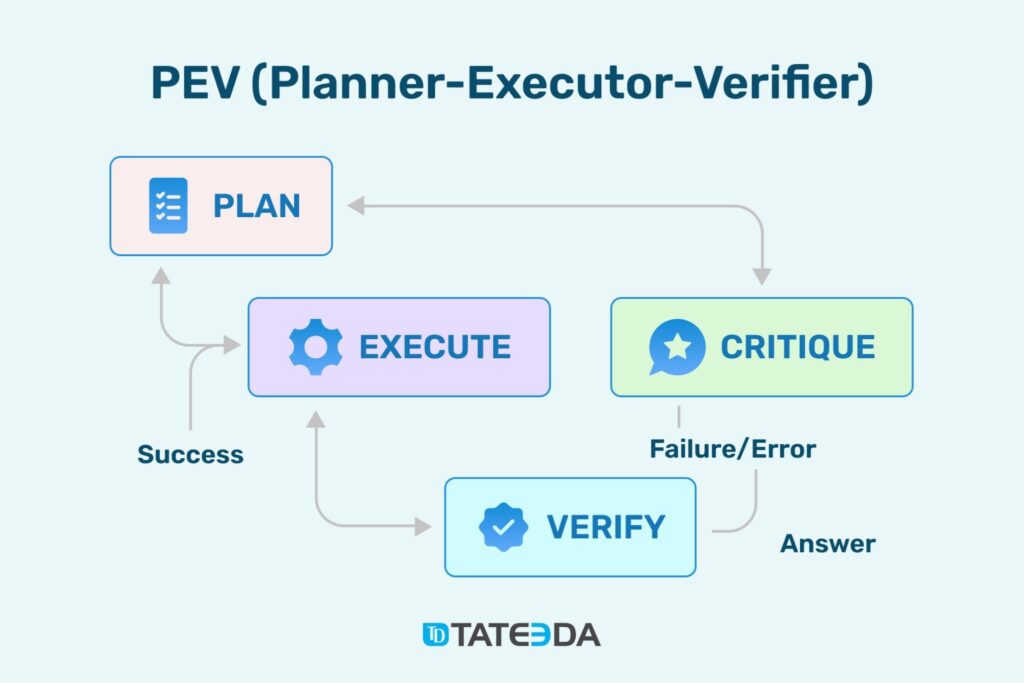
PEV workflow overview: planner sets steps, executor runs tools, critique scores quality, verifier checks results before release.
The Verifier checks results against rules and policies, then either returns an answer or routes the work back for a fix. This is the essence of PEV agent architecture for HIPAA-compliant apps. Teams that want a fast start often engage PEV AI agent development services to stand up the first pilots with proper logging, approvals, and kill switches.
Where PEV agents fit and how they deliver value:
- Clinical documentation copilot. A PEV healthcare AI assistant for EHR integration ingests a transcript, reads meds, allergies, and vitals via FHIR, drafts a structured SOAP note, then verifies required fields, code alignment, and interaction checks before saving a draft for sign-off. This is also a strong pattern for PEV AI agents for clinical documentation and ambient scribing that target note quality and time reduction.
- Triage and symptom intake. This is how to build PEV agents for clinical workflows that ask adaptive questions, call guideline libraries, and verify red-flag thresholds before proposing a disposition. The agent can schedule a slot or open a secure message so patients move faster and staff avoid repeat intake.
- Prior authorization and eligibility. PEV agents for prior authorization and eligibility checks assemble payer-specific artifacts, fetch labs and imaging, map ICD and CPT, verify criteria and completeness, then submit with provenance. Teams see fewer pends and shorter determination times.
- Revenue cycle and coding. PEV agents for revenue cycle management and coding support propose CPT and ICD from documentation, execute NCCI edits, validate payer rules, and package the claim with evidence links. Finance gains a higher first-pass yield and less denial rework.
- Remote patient monitoring. PEV multi-step AI agents with SMART on FHIR connectivity analyze wearable streams, build baselines, detect outliers, and verify against medication lists and care protocols. Low-value alerts are suppressed, and high-risk events open tasks with traceable evidence.
- Clinical trial or referral matching. The agent checks for inclusion and exclusion, queries registries, verifies compliance with criteria, and returns a clinician-ready summary with sources. Patients can access suitable studies sooner, and care teams save hours on manual searches.
- Workforce and HR in care settings. Nearshore PEV AI agent development for U.S. companies can automate credential checks, schedule optimization, and timekeeping validation with auditable proofs so operations run predictably and compliance gaps shrink.
Evidence and Market Signals for AI (PEV) Agents
The buying climate is shifting toward auditable automation. Medicare Advantage processed nearly 50 million prior-auth requests in 2023, with 6.4% denied, per KFF analysis, and KFF enrollment shows 54% of Medicare beneficiaries are now in MA plans, so any efficiency gain scales fast.
The FDA draft on AI for regulatory decisions favors transparent, provable logic. Provider tools are maturing as KLAS 2025 highlights strong satisfaction with ambient documentation. Budgets are following, with PwC survey data showing most U.S. executives increasing AI spend and many already adopting agents.
In this context, PEV agents resonate because they turn high-volume friction, such as:
- Re-keying the same patient or authorization data across portals
- Chasing missing attachments on many prior auths
- Fixing the same coding edit on large batches of claims
- Manually triaging similar intake messages every morning
- Checking status on dozens of claims across payer sites.
into outcomes that matter: faster decisions before care is delayed, cleaner first-pass claims, quicker scheduling from structured intake, fewer status-chasing clicks for staff, and auditable traces that help compliance teams sleep at night.
Quick view: additional workflows PEV can automate
| Use case | Workflow stage | Primary data | PEV focus | Outcome |
| Discharge instructions | Post-visit | Orders, meds, education | Retrieve context; verify literacy and language | Safer handoffs |
| Care-gap closure | Population health | Registries, measures | Plan queries; verify attribution | Higher compliance |
| Imaging follow-ups | Radiology ops | Reports, scheduling | Extract findings; verify callbacks | Fewer misses |
| Medication refills | Pharmacy ops | Med lists, vitals | Interaction checks; adherence logic | Fewer errors |
| Claim status checks | RCM ops | Payer APIs | Plan inquiry; verify codes | Faster resolution |
| Referral routing | Network ops | Directories | Filter match; insurance checks | Shorter waits |
| Social needs flags | Care management | SDOH data | Verify screening thresholds | Better coordination |
| Device onboarding | RPM setup | Device clouds, FHIR | Verify linkage and consent | Fewer setup failures |

PEV Agent Architecture and Integrations for EHR and Payers
Think of a PEV agent as a small, governed “helper” that sits between your clinical systems (EHRs) and payer systems. It plans a task, calls the right systems, and then finalizes the results after verification. In healthcare, this helper must speak the common data languages—FHIR R4 for modern APIs and HL7 v2 for legacy feeds—and it must demonstrate its actions for audit and safety purposes.
There are two practical ways to deploy it. For point-of-care features, embed a PEV healthcare AI assistant for EHR and wearables integration that launches from the chart using SMART on FHIR. It inherits the user and patient context, reads the minimum data needed, and returns a draft or task for human review. For background work (e.g., assembling prior-auth packets overnight), run the agent as a sidecar service and use SMART Backend Services to authenticate server-to-server with narrow permissions.
How the data pieces fit, in plain terms: FHIR R4 is a modern, web-style API where “resources” like Patient, Medication, or Observation are readable and writeable in predictable formats. HL7 v2 is a long-standing messaging pipe that many hospitals still use for admissions, results, and orders; the agent can translate those messages into its internal model (or into FHIR) so the Planner always has fresh signals without heavy polling. Payer connections come in two forms: FHIR-based APIs, where available, and clearinghouse EDI/X12 transactions (270/271 eligibility, 278 prior auth, 276/277 status, 835 remittance, 837 claims) for broad reach.
Identity and consent are the guardrails. For user-driven flows, request only the SMART scopes you truly need (for example, patient/Observation.read instead of a blanket patient/*.read). For server-side runs, attach a clear “purpose of use” and link to a Consent record so auditors can see why the agent touched PHI. Map Practitioner and Organization roles to least-privilege service identities, and keep tokens short-lived. This keeps the PEV agent architecture for HIPAA-compliant apps small, explainable, and approvable by security teams.
A PEV agent isn’t “just a chatbot.” It’s an orchestrator with contracts. Each tool adapter declares what it expects in and what it will return (schemas, not prose). The Verifier is a bundle of deterministic checks—payer edits, clinical rules, schema validations—that produce a clear pass or fail with reasons. If a step can’t prove what happened (sources, parameters, results), the agent doesn’t proceed. That design is what turns an idea into something safe to run in production.
Here’s a simple map of the standards in everyday language:
| Standard | Plain English | Typical Use in PEV |
| FHIR R4 | Modern API for clinical data | Read context for planning; write drafts, tasks, and messages |
| HL7 v2 | Event messages from hospital systems | Feed admissions/results/orders into the Planner in near-real time |
| SMART on FHIR | Secure app launch with user/patient context | An interactive assistant inside the EHR with minimal scopes |
| SMART Backend Services | Server-to-server access pattern | Unattended jobs like bulk evidence assembly or status checks |
| EDI/X12 | Transactions for payers/clearinghouses | Eligibility, prior auth, claim status, claims, remittance |
What this unlocks for non-technical leaders: you can start small and measurable. For example, a documentation agent can draft a SOAP note, attach provenance, and park it as a DocumentReference for sign-off—no silent writes.
A prior-auth agent can pre-assemble lab values and imaging, check plan-specific rules, and create a Task with all attachments ready. A coding agent can validate NCCI edits and package a clean claim, then post status updates when 276/277 responses arrive. These are tangible, low-risk wins that reduce back-and-forth and make audits straightforward.
To keep it reliable after go-live, add lightweight observability: traces of tool calls, verification results, and a dashboard for pass rates and turnaround times. Pair that with kill switches, rate limits, and idempotent writes so operations stay calm during outages. When you’re ready to expand, you don’t “rewrite”—you add another adapter or another verified step. That’s why many teams use PEV AI agent development services to set up the initial rails, then grow coverage sprint by sprint.
High-Impact Use Cases with Sample Step Lists
These examples show how a PEV agent operates in real workflows. Each starts small, uses clear data contracts, and ends with a draft or submission that a human can review. The point is not “full autonomy,” but reliable steps you can audit.
1) Clinical documentation copilot (SOAP note from visit audio)
A PEV healthcare AI assistant for EHR integration runs inside the chart, so context is already in scope:
- Planner: Define note structure, required fields, and sources. List FHIR reads for meds, allergies, vitals, and problems.
Executor: Transcribe the encounter, retrieve FHIR resources, and generate a structured SOAP draft with coded problems where possible. Create a DocumentReference and a Task for review. - Verifier: Check required fields, problem–code alignment, and medication consistency. Confirm timestamps and clinician identity. Flag any uncertainty.
- Output: A ready-to-sign draft plus a short evidence panel. Clinicians edit or accept, then the agent archives provenance for audit.
Why it helps: fewer addenda, faster closeout, and note quality that is explainable. This pattern also generalizes to consult letters and discharge summaries.
2) Prior authorization packet builder (imaging example)
For payer requests, PEV agents for prior authorization and eligibility checks shine because the criteria are explicit:
- Planner: Identify CPT, ICD, payer, and plan rules. List evidence needed: prior imaging, notes, labs, and guideline citations.
- Executor: Pull artifacts from the EHR, attach reports, and extract key values. If the plan supports APIs, prepare a FHIR PriorAuth; if not, assemble a 278 transaction via the clearinghouse.
- Verifier: Validate clinical criteria, attachment completeness, code compatibility, and member eligibility. Attach a pass/fail reason set.
- Output: A submission-ready packet with provenance. On failure, open a Task to request missing items from staff.
Why it helps: fewer pend letters and predictable cycle times. You can start with one modality and one payer, then expand coverage.
3) Revenue cycle support (codes, edits, and clean claims)
PEV agents for revenue cycle management and coding support reduce avoidable denials:
- Planner: Define the target claim, required code sets, and payer edit rules.
- Executor: Propose CPT and ICD from documentation, apply NCCI edits, and attach required evidence. Create a draft 837 or populate claim objects through your clearinghouse API.
- Verifier: Enforce code pair rules, modifier logic, and medical necessity hints. Confirm member and provider identifiers.
- Output: A clean claim bundle with an explanation of changes and links back to evidence.
Why it helps: higher first-pass yield and less time spent chasing edits after submission.
4) Remote patient monitoring (signals into tasks, not noise)
For wearables and home devices, PEV multi-step AI agents with SMART on FHIR connectivity keep alerts meaningful:
- Planner: Set per-patient baselines, signal windows, and escalation rules.
- Executor: Ingest device data, normalize units, and compute rolling trends.
- Verifier: Compare outliers to baselines, medication lists, and protocol thresholds. Suppress low-value alerts, open a task for high-risk events, and add a clinician-ready summary.
- Output: Actionable tasks with evidence graphs and clear next steps.
Why it helps: less alarm fatigue and faster intervention on the cases that matter.
5) Intake to scheduling (from messages to booked slots)
This is a friendly on-ramp for teams new to agents:
- Planner: Define the questions needed to triage the request.
- Executor: Structure patient-reported data, propose a disposition, and query calendars.
- Verifier: Apply screening rules, eligibility checks, and location constraints.
- Output: A proposed slot or a routed message with all context attached.
Why it helps: fewer back-and-forth messages and a faster time to the appointment.
“A few build notes for leaders: start with one workflow and one system of record, then widen. Add PEV agent verification and governance best practices early, so approvals are smooth. If you want a faster path, lean on PEV AI agent development services for the first adapter and verifier suite, then let your team clone the pattern across service lines. This is how to build PEV agents for clinical workflows that stay reliable after go-live without overwhelming your stack.”
— Slava K. TATEEDA’s CEO
How PEV AI Agents Are Built: Methods and Technologies
A helpful way to think about Planner–Executor–Verifier (PEV) agents in healthcare is to see them not as a single monolithic “AI,” but as a small system with clear responsibilities: a Planner that turns a request into steps, an Executor that performs those steps using approved tools, and a Verifier that checks results against rules before anything is committed back to clinical or payer systems. The magic isn’t only in the model; it’s in the contracts between these parts and in the predictable interfaces to EHR and payer rails. For distributed care models, this same pattern underpins custom telemedicine software development solutions, where the agent coordinates remote intake, device data, and clinician messaging without losing auditability.
Under the hood, the Planner is typically an LLM guided by strict instructions plus a tiny domain language (a few JSON fields are enough) that describes the step list, inputs, outputs, and guardrails. The Executor is not “free-form AI” at all; it is a library of adapters—FHIR R4 for clinical data, HL7 v2 listeners for events, SMART on FHIR for contextful launch, and EDI/X12 for claims, status, and prior auth—that transform the plan into real API calls with least-privilege credentials. The Verifier is a test harness: a set of deterministic checks (schema validation, payer edits, clinical rules, identifier matching) that return a crisp pass/fail with reasons, which is why this pattern maps so well to PEV agent architecture for HIPAA-compliant apps. Teams that provide custom EHR/EMR software development services often expose these standards-based adapters first, because reliable connectivity is what lets a PEV agent do useful, traceable work.
Typical layers you’ll see in a production-ready PEV build:
| Layer | Role in the agent | Common tech/standards | Notes for leaders |
| Planning | Turn intent into steps | LLM + small JSON/DSL; prompt templates | Keep the plan machine-readable, not prose. |
| Retrieval & context | Bring the right facts | Role of the agent | Limit scope; attach sources for provenance. |
| Tool adapters | Do the work safely | FHIR R4, HL7 v2, SMART on FHIR, EDI/X12 | Each adapter declares inputs/outputs as schemas. |
| Verification | Prove it’s correct | Rule engine, JSON Schema, payer edit sets, clinical checks | Deterministic; no prompts here. |
| Identity & access | Keep risk low | OAuth 2.0/OIDC, SMART scopes, service accounts | Short-lived tokens, role scoping, audit logs. |
| Observability | See what happened | Traces/metrics/logs; provenance records | Tie dashboards to business KPIs. |
If you’re wondering how to build PEV agents for clinical workflows in practical terms, the strongest habit is to design the contracts first and the prompts second. Define each step’s input and output as JSON, enforce them with validators (e.g., JSON Schema or typed models), and write the Verifier’s rules as executable tests, because this makes failures actionable and keeps humans in the loop with clear reasons.
For example, a PEV healthcare AI assistant for EHR integration can only write a draft note if the required_fields_check passes; a PEV agent for prior authorization and eligibility checks can only submit a packet if attachments_complete and criteria_met both pass; and PEV agents for revenue cycle management and coding support will refuse to package a claim until ncci_edits_ok is true.
To keep things reliable over time, add PEV AI agent MLOps: monitoring, drift control, and rollback. That usually means capturing acceptance rates of each Verifier test, alerting on unusual failure patterns, and keeping a safe rollback path for any model or rule change that might affect outcomes. Because planners change and payers evolve, these counters are less “nice-to-have” and more the way you prevent silent regressions.
On the patient-facing side, the very same governance helps when agents power custom patient portal software solutions, where a draft message, visit summary, or refill request must include provenance so clinicians can quickly trust and approve it.
A small checklist many teams adopt:
- Write the step contracts first, then wire the prompts to produce exactly those shapes.
- Treat every adapter like a public API: version it, test it, and prove idempotency for writes.
- Keep SMART scopes narrow; prefer resource-specific scopes over wildcards.
- Store provenance (sources, parameters, decisions) with each result so audits are boring, not stressful.
- Put the “Critique” before the Verifier when quality or safety warrants a second look.
- Fail loudly and early: on fail, re-plan a smaller step or escalate with evidence.
Finally, choose technologies that play nicely with standards rather than bending standards around your stack. PEV multi-step AI agents with SMART on FHIR connectivity remain maintainable precisely because they rely on predictable rails—FHIR resources for context and drafts, HL7 v2 for signals, and well-scoped identities for every call—so clinicians see helpful drafts instead of surprises, finance gets cleaner transactions rather than guesswork, and compliance teams can approve the system with confidence.
Final Word: Get PEV AI Agents Integrated for Healthcare
Planner–Executor–Verifier (PEV) agents in healthcare turn disorganized, vague, multisystem work into clear steps that are planned, executed with approved tools, and verified before anything touches the record. You get faster decisions, fewer rework loops, and audit-ready traces your compliance team can trust.
TATEEDA can help. We are nearshore custom software development providers in San Diego with HIPAA-grade delivery and deep integrations across FHIR R4, HL7 v2, SMART on FHIR, and payer EDI/X12. Our team designs PEV agent architecture for HIPAA-compliant apps and ships measurable outcomes through PEV AI agent development services.
If you are ready to automate documentation, prior authorization, coding, RPM, or patient-facing flows, let’s translate your goals into a small, testable PEV workflow that is easy to explain, easy to audit, and ready to scale.