The Architecture of Value: How to Stop Leaking ROI in Healthcare IT

Slava Khristich



Vlad Nazarov

In this article, we explore how healthcare organizations can maximize their IT return on investment by moving beyond simple feature acquisition to focus on architectural integrity, technical debt reduction, and strategic automation. By addressing common pitfalls like cloud waste and fragmented legacy systems, leaders can transform their digital health applications from costly overhead into streamlined, high-performing assets that serve both staff and patients more effectively.

If you require technical assistance to optimize ROI across your healthcare software infrastructure, please contact our health tech experts for individualized project consultation!
Healthcare IT spending rarely fails because leaders do not care. It fails because systems become tangled, cloud bills swell quietly, legacy code resists change, and every “small update” drags five other problems into the room. A patient portal goes live, but support tickets rise. A billing workflow is digitized, but staff still re-enter the same data in three places. An EHR-connected tool looks promising, then turns brittle under compliance, audit, and maintenance pressure.
That is where ROI gets lost.
In healthcare, return on investment is not just about launching software. It is about building digital health applications that cost less to run, ask less of staff, fit regulatory expectations, and remain workable a year later when the team needs new features, a new integration, or a security update. Better architecture helps. So do cleaner cloud configurations, lower technical debt, careful use of AI in healthcare operations, and sensible modernization of aging systems.
This article breaks down where healthcare IT ROI tends to leak, what practical fixes matter most, and how organizations can simplify complex environments without trading speed for compliance.
What makes TATEEDA qualified to discuss ROI in the healthcare sector?
TATEEDA’s credibility in discussing Healthcare IT ROI is grounded in a decade of experience delivering and maintaining HIPAA-grade systems for U.S. organizations. This includes supporting high-throughput platforms for major providers, such as operating a platform for AYA Healthcare that serves thousands of users daily under strict HIPAA regulations.
This hands-on experience has provided TATEEDA with deep insight into the real-world bottlenecks and expensive friction points—such as staff credentialing, complex scheduling, and compliance reviews—where operational value is typically lost.
Unlike vendors who focus purely on feature count, TATEEDA’s approach aligns with the core architectural and financial arguments presented in this article. They leverage nearshore development and use AI-assisted practices to accelerate the software delivery cycle by up to 3–4 times, which is a direct mechanism for improved development ROI.
Furthermore, their expertise in integrating AI for medical workflow automation, refactoring legacy code, and working with complex standards like FHIR and HL7 demonstrates a practical understanding of how to build digital health assets that are cheaper to run, easier to integrate, and designed to lower long-term maintenance overhead.
Table of Contents
Why healthcare IT ROI often falls short
Many healthcare organizations do not suffer from a lack of software. They suffer from too much disconnected software, too many handoffs, and too many decisions made for short-term convenience.
A familiar pattern appears:
- One vendor builds a patient-facing layer
- Another handles billing logic
- A third manages reporting
- Internal teams patch integrations over time
- Nobody fully owns the architecture anymore
The result is expensive friction. Simple workflow changes turn into engineering projects. Cloud resources remain oversized because nobody wants to risk downtime. Old modules stay in place because replacing them looks painful.
Technical debt compounds quietly, then all at once. Here are some of the most common reasons ROI stays weak:
- Fragmented systems with duplicate functions
- Legacy code that is difficult to understand or test
- Overbuilt cloud environments with idle resources
- Compliance fixes added late instead of early
- Poor interoperability planning
- User interfaces that do not match clinical or administrative reality
- Support and QA effort that keeps rising after launch
Healthcare organizations often feel this problem before they name it. Releases slow down. Change requests start sounding expensive. Engineers avoid touching certain modules. Staff use spreadsheets as survival tools. Rather than being a mark of software achievement, such inefficiencies represent a significant hidden expense.
What ROI in healthcare IT actually means
ROI in healthcare software development should be measured more broadly than direct revenue. Sometimes the win is obvious, like faster patient collections or stronger appointment conversion. Just as often, the win is quieter but equally important: lower support burden, fewer failed claims, less duplicate data entry, or a codebase that no longer fights every release.
A stronger ROI picture often includes the following:
| ROI factor | What it looks like in practice |
| Lower operational cost | Fewer manual tasks, less repetitive admin work, lower support hours |
| Lower infrastructure spend | Right-sized cloud services, less idle capacity, better storage policies |
| Faster delivery | Engineering teams spend less time untangling old code |
| Better staff productivity | Fewer clicks, fewer duplicate workflows, cleaner interfaces |
| Lower error rates | Better validation, cleaner integrations, fewer billing or documentation mistakes |
| Longer system life | Existing platforms remain usable without constant patchwork |
Healthcare leaders sometimes chase visible features when the larger financial picture sits elsewhere. A simple architectural fix that removes duplicate processing may create more lasting value than a flashy front-end upgrade.
A refactoring initiative that cuts release friction may outperform a new dashboard. The point is straightforward: ROI rises when systems become easier to operate, easier to change, and less expensive to carry.
Win the long-term financial argument: Start with architecture
Healthcare IT projects often get pulled toward features first. That is understandable. Features are easy to demo. Architecture is harder to sell in a meeting. Yet architecture is where the long-term financial argument is won or lost.
A strong architectural foundation does a few plain but powerful things:
It reduces repeated work
When systems share data cleanly, teams stop rebuilding the same logic in different places. Patient details, billing states, care updates, and device data do not need to bounce through manual correction loops.
It makes integrations less painful
Healthcare systems live among EHRs, patient portals, scheduling tools, payment systems, device feeds, and internal reporting layers. If the application structure is chaotic, every new connection becomes a fragile custom job.
It lowers future change cost
Modular application design, clear service boundaries, and disciplined data flows give teams a better chance of changing one part without breaking three others.
That does not mean every project needs a dramatic rebuild. It does mean leaders should ask the right questions early:
- Where does business logic live?
- Which modules create the most release fear?
- Can core functions be updated independently?
- Are integrations clean or heavily patched?
- Is the data model understandable to new engineers?
Those questions sound technical, but they are financial questions in disguise.

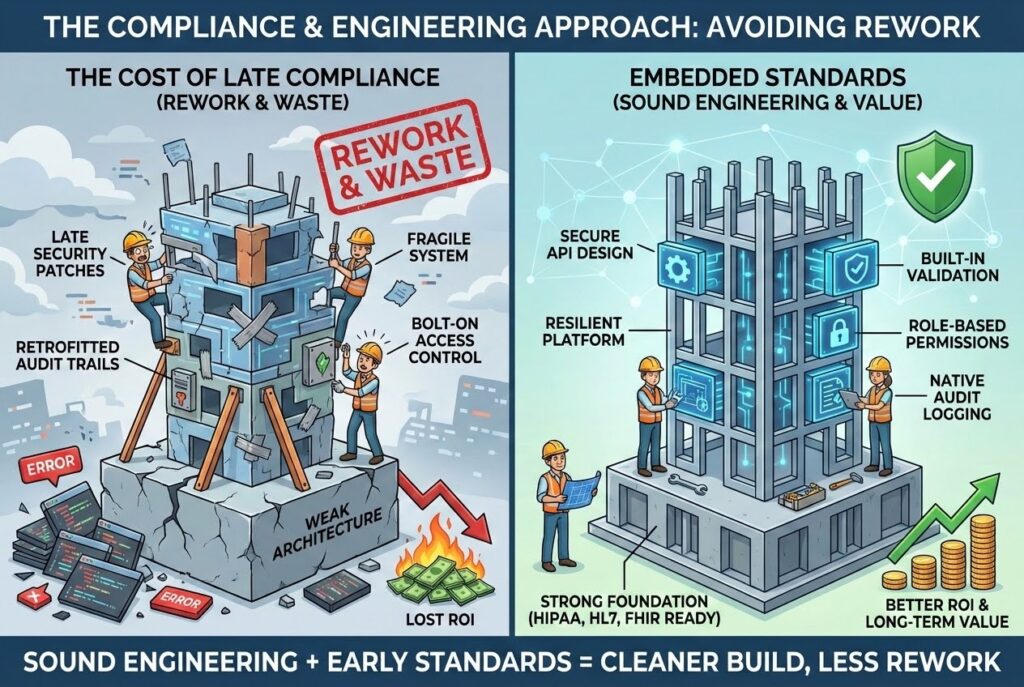
Use standards and sound engineering to avoid rework
In healthcare, weak compliance planning does more than create regulatory risk. It creates waste.
When audit trails, role-based access, secure data handling, and interoperability requirements are treated as late additions, teams end up rewriting work they already paid for. That is a bad habit, and an expensive one.
The cleaner path is to embed healthcare-specific expectations into the build from the start. That includes:
- HIPAA-aware access control
- logging and audit visibility
- encryption practices appropriate to the system
- secure API design
- HL7 or FHIR readiness where needed
- validation rules for sensitive workflows
- clear user permissions by job role
These are not decorative checkboxes. They shape how a system behaves under pressure. A patient portal, for example, should not require heavy retrofitting to support secure messaging, access boundaries, payment features, or medical document visibility. An RPM platform should not need structural surgery when device data volume grows or access rules become stricter.
When healthcare standards influence architecture from the beginning, teams avoid much of the late-stage rework that quietly damages ROI.
Cost-efficient cloud configurations matter more than many teams admit
Cloud waste is rarely dramatic. It is cumulative.
One oversized instance. A forgotten environment. Logging is set up far beyond practical need. Storage classes that never change. Containers running around the clock for workloads that barely move. None of these looks catastrophic in isolation. Together, they can distort the cost structure of a healthcare platform.
That matters because digital health products often carry a mix of variable demands:
- Patient portals may have uneven traffic
- Administrative workflows peak at predictable hours
- Device data pipelines may fluctuate
- Reporting jobs can spike resource use at specific times
- Test and staging environments may be active far less than production.
A cost-aware cloud review should examine:
Compute sizing
Do workloads actually justify the current instance mix, container count, or node allocation?
Storage behavior
Is clinical or operational data staying in expensive storage longer than necessary? Are lifecycle rules in place?
Environment sprawl
How many test, QA, demo, and backup environments exist, and which of them are truly needed?
Monitoring cost
Observability is essential, but indiscriminate log collection can become a budget issue of its own.
Availability decisions
Some systems need extremely high resilience. Some do not. Treating every component the same can inflate spending without proportional gain.
Below is a practical view:
| Cloud cost issue | Typical cause | ROI-friendly response |
| Oversized compute | Safety-first provisioning left untouched | Review actual workload patterns and resize |
| Idle environments | Old QA, staging, or demo systems kept alive | Schedule shutdowns or retire unused environments |
| Storage bloat | No retention logic or lifecycle policy | Move older data to lower-cost storage tiers |
| Excess logging | Collecting everything forever | Keep what supports security, audits, and troubleshooting |
| Uniform availability design | Applying premium resilience to every service | Match architecture to business and compliance need |
AI can make healthcare operations more cost-efficient
A lot of AI talk in healthcare floats at the level of slogans. ROI comes from the opposite: narrow, specific, supervised uses that remove routine effort and shorten response time inside the organization.
AI can support cost efficiency in healthcare operations when it is applied to areas like:
- document classification
- structured data extraction
- internal search across policies or knowledge bases
- triage of support tickets or requests
- anomaly detection in operational workflows
- billing support tasks
- appointment or communication routing
- summarization of repetitive internal content.
The strongest uses usually share three traits:
- They target high-volume repetitive work.
- They keep humans in control of sensitive decisions.
- They are measured against time saved, error reduction, or staff relief.
That last point matters. Custom AI solutions should not be introduced because it sounds modern. It should be introduced because it reduces drag.
For example, an internal operations team might use AI to classify incoming requests, extract fields from repetitive documents, or surface relevant policy information faster. A revenue cycle function might use AI assistance to reduce manual review time for structured inputs. A support team might use it to draft responses, summarize issues, or route requests more accurately.
In regulated settings, discipline matters. Sensitive actions still need human approval. Clinical interpretation, diagnosis, orders, and other high-risk outcomes are not areas for casual automation. But routine operational load? That is where AI can genuinely trim costs.
Refactoring legacy code with AI copilots can reduce maintenance burden
Legacy systems are expensive in a particular way: they waste attention. Engineers spend hours understanding brittle logic, tracing unclear dependencies, and guarding against breakage in modules nobody fully trusts.
This is where AI copilots can be useful, provided the work stays under senior review.
They can help teams:
- Inspect repetitive code patterns faster
- Draft documentation for underexplained modules
- Identify duplicated logic
- Suggest test cases around weak coverage areas
- Accelerate low-risk refactoring work
- Flag unused functions, risky dependencies, or suspicious patterns
That does not mean AI should rewrite a regulated healthcare system unchecked. It should not. But as an assistant inside a supervised modernization effort, it can reduce the cost of moving legacy code into a healthier state.
A good modernization path often looks like this:
Step 1: Identify high-friction modules
Focus on code that causes release delays, incident risk, or support burden.
Step 2: Improve visibility
Use static analysis, dependency review, and AI-assisted code understanding to map what the system is actually doing.
Step 3: Add test protection
Before major changes, strengthen coverage around risky workflows.
Step 4: Refactor in phases
Replace duplicated logic, simplify module boundaries, and retire dead code gradually.
Step 5: Keep human review central
In healthcare, every AI-suggested change still needs engineering judgment, especially where privacy, access, billing, or patient-related workflows are involved.
This approach is usually more financially sensible than a dramatic rewrite. Full replacement has its place, but selective modernization often creates a better balance of speed, control, and cost.

Technical debt is not abstract. It is a monthly overhead.
Technical debt gets discussed so often that it can start sounding philosophical. In practice, it is concrete. It shows up in time, money, fear, and delay.
You are likely dealing with meaningful technical debt when:
- Minor changes require heavy regression testing
- Engineers hesitate to edit certain modules
- Onboarding new developers takes too long
- Bug fixes trigger unrelated issues
- Release preparation becomes a long, manual ritual
- Data logic is duplicated across systems
- User complaints keep tracing back to old architectural choices
Technical debt reduces ROI because it imposes costs on every future move. It makes every new feature more expensive. Every integration takes longer. Every compliance adjustment lands harder. Even cloud costs can rise because old code and architecture often waste resources together.
A practical debt-reduction agenda usually includes:
- refactoring the modules with the highest maintenance burden first
- removing duplicate logic across services or components
- tightening test coverage around sensitive workflows
- simplifying data models where possible
- documenting critical business rules
- retiring code paths and integrations that no longer serve a clear purpose.
Below is a simple prioritization model:
| Priority area | Why it matters |
| Modules linked to patient data, payments, or access control | High business and compliance impact |
| Code that slows every release | Multiplies cost across the whole team |
| Legacy integrations patched repeatedly | Common source of hidden support burden |
| Functions with weak test coverage | Higher risk during any change |
| Duplicate business logic | Causes inconsistency and repeated maintenance |

The point is simple: technical debt should sit on the financial agenda, not just the engineering agenda.
Best practices that improve ROI in digital health applications
A few habits repeatedly separate healthier healthcare IT systems from expensive ones.
Map workflows before writing code
Many costly systems were built around assumptions, not observed workflows. Understand how patients, staff, coordinators, and administrators actually use the process.
Reduce duplicate entry
If data must be entered repeatedly across billing, patient, and operational tools, the system is creating cost, not reducing it.
Build for interoperability early
Late integration work is often messy, expensive, and disruptive. It is better to plan for the connection from the beginning.
Keep interfaces plain and usable
A confusing staff-facing tool can erase the value of strong back-end work. Click count matters. Clarity matters. Friction matters.
Review cloud usage regularly
Cloud cost should be treated as an active operating concern, not a passive invoice.
Keep refactoring on the roadmap
Debt does not disappear because teams are busy. In fact, busy teams usually pay more for postponing it.
Where healthcare organizations can often find ROI first
Some systems are especially worth reviewing when ROI feels weak:
- patient portals with low engagement and high support effort
- EHR-connected tools with brittle integrations
- remote patient monitoring platforms with costly data handling
- billing and payment portals with failed transactions or manual follow-up
- intake and scheduling systems with duplicate steps
- internal admin tools held together by spreadsheets and staff memory
- legacy platforms that consume a disproportionate share of engineering time
These areas often carry both operational friction and architectural problems. That makes them strong candidates for ROI-focused cleanup.

A practical checklist before funding the next IT initiative
Before approving another platform upgrade, rebuild, or digital health application, ask:
- Are we solving a real workflow problem or adding another layer?
- Which part of the current system creates the most recurring cost?
- Are cloud resources aligned with actual usage?
- Where is technical debt slowing change?
- Can AI remove repetitive internal work safely?
- Are compliance controls part of the design, or are they being patched on later?
- Will this system be easier to live with two years from now?
Those questions are not glamorous. They are useful. Useful questions tend to produce better ROI.
Final thought
Healthcare IT ROI does not rise because a team bought more software or added more features. It rises when systems become simpler to run, less costly to maintain, and less dependent on fragile workarounds. Proven architecture, healthcare-aware engineering, cost-conscious cloud decisions, disciplined use of AI, legacy refactoring, and technical debt reduction all matter here.
That is the real opportunity. Not more system sprawl. Less waste.
And in healthcare, where compliance pressure, staffing pressure, and operational pressure rarely ease up, that kind of clarity can make a very large financial difference over time.
For organizations ready to take action on these architectural and financial arguments, TATEEDA serves as a strategic partner. With a decade of experience in HIPAA-grade system delivery and maintenance, our firm focuses on turning costly legacy systems into streamlined, high-performing assets.
We help improve ROI by leveraging nearshore teams and AI-assisted development practices to accelerate software delivery by 3–4 times, and by applying expertise in AI-driven workflow automation, legacy code refactoring, and secure integration with complex standards like FHIR and HL7. This holistic approach ensures digital health applications are cheaper to run, easier to integrate, and designed to reduce long-term maintenance overhead.