EHR Medication Management Module: eRx, Refill Requests, Drug Database Integration, and Patient Safety Logic

Slava Khristich

Vlad Nazarov

This article explains what it takes to build an EHR medication management module that works safely in real clinical and pharmacy workflows. You’ll learn how eRx, EPCS, refill requests, drug database integration, allergy checks, drug-drug interaction logic, FHIR medication resources, and audit controls fit together inside one medication lifecycle.
If your team is planning a new medication module, rebuilding legacy prescribing software, or connecting EHR workflows with pharmacies, this guide will help you understand which technical decisions matter before development begins, where compliance risks appear, and how to avoid architecture gaps that can affect clinicians, pharmacists, and patients.
Medication management is one of the highest-risk areas of EHR software development. A prescribing screen may look simple, but the system behind it must handle clinical decision support, pharmacy messaging, controlled-substance rules, patient refill workflows, drug database updates, allergy logic, audit trails, and external service failures.
If your engineering team is building or extending an EHR medication management module, the difficult work sits in four connected subsystems:
- electronic prescribing, or eRx;
- controlled-substance signing, or EPCS;
- refill request handling;
- drug database integration and patient safety logic.
A module that works in a test environment can still fail in production if it cannot process pharmacy responses, distinguish refill sources, keep drug knowledge current, separate allergy rules from interaction rules, log overrides, or recover when an eRx network, drug database, EPCS service, or PDMP connection is unavailable.
This article explains the architecture behind a safe, production-ready medication management module. It covers electronic prescribing EHR workflows, EPCS compliance, NCPDP SCRIPT integration, FHIR R4 medication mapping, drug database integration, drug-drug interaction checks, refill routing, clinical decision support, audit logging, and failure handling.
For teams planning a broader EHR build, see TATEEDA’s EHR and EMR software development services.
Key takeaways:
- EPCS is required when controlled substances are prescribed electronically. It is not just “MFA for prescriptions.” It involves identity proofing, two-factor signing, logical access control, application audit or certification, record retention, and controlled-substance-specific workflows.
- NCPDP SCRIPT is the main prescription transaction standard used for U.S. eRx workflows such as new prescriptions, renewal requests, change requests, cancellations, fill status, medication history, long-term care, and electronic prior authorization. Confirm the required SCRIPT version and message scope with the network or certification program for the exact integration.
- FHIR R4 MedicationRequest is useful for representing medication orders inside EHR, care coordination, patient-facing, analytics, and downstream integration workflows. It does not replace NCPDP SCRIPT for pharmacy-routing transactions.
- Public drug datasets such as RxNorm, DailyMed, FDA labeling data, and Orange Book information are useful, but they do not replace a licensed clinical drug knowledge source for production safety checks.
- Drug-drug interaction checks and drug-allergy checks should not share one generic “safety check” path. They use different source data, matching logic, clinical semantics, severity rules, and override policies.
- Refill workflows must separate pharmacy-originated renewal requests from patient-initiated portal requests. They arrive through different channels and should not be processed as the same event.
- HIPAA requires appropriate safeguards for ePHI, but it does not prescribe one universal AES, TLS, or audit-log retention setting for every medication system. Security controls need to follow risk analysis, organizational policy, contracts, and applicable regulations.
- Pregnancy and lactation alerts should not rely on old FDA A/B/C/D/X pregnancy categories for current prescription labeling. Modern medication safety logic should use updated pregnancy and lactation labeling content, structured clinical context, and drug database guidance.
Why is TATEEDA qualified to explain EHR medication management architecture?
TATEEDA works with healthcare and pharmaceutical organizations on software systems where medication, claims, patient access, workflow state, and secure data handling intersect. That experience is directly relevant to EHR medication management because prescribing software is not just a form inside a clinical interface. It depends on safe workflow routing, third-party integrations, transaction history, exception handling, audit events, and patient-facing communication.
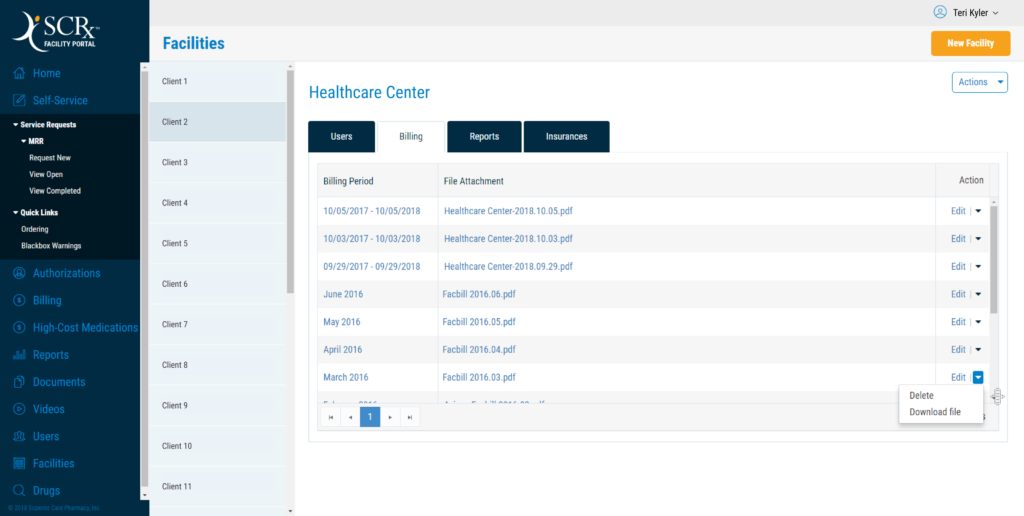
One relevant example is TATEEDA’s SCRx pharmacy claim processing and medication fulfillment project. The system supported pharmacy claim processing, medication fulfillment workflows, backend development, cloud integration, third-party API integration, bulk PDF import, OCR, system alerts, and operational automation. Those patterns matter in medication management modules because refill handling, pharmacy responses in medication management modules because refill handling, pharmacy responses, prescription-related queues, and failure recovery require the same kind of durable workflow design.
Another relevant example is TATEEDA’s pharmaceutical business automation platform, built to support ordering, processing, and shipping prescription drugs for business partners. This kind of project gives practical context for prescription-adjacent operations: structured product data, order states, partner workflows, data management, and controlled process visibility.
Together, these case studies do not replace clinical pharmacy validation or EPCS certification work. They show relevant engineering experience with pharmacy workflows, healthcare data exchange, patient and business portals, API integrations, document processing, alerts, and audit-conscious system design, which are core building blocks of a reliable EHR medication management module.
Table of Contents
What an EHR medication management module actually handles
A medication management module in an EHR software system is not a simple prescription pad. It is a state machine for the medication lifecycle.
At minimum, it should support:
- Medication selection
A clinician selects a drug, dose, route, frequency, quantity, days’ supply, pharmacy, refills, and patient instructions. - Clinical review
The system checks allergies, active medications, duplicate therapy, age, weight, renal function, pregnancy or lactation context, formulary status, and prior authorization needs where data is available. - Order signing
The prescriber signs the order. If the medication is a controlled substance and will be sent electronically, EPCS controls apply. - Transmission
The prescription is routed to a pharmacy through an approved eRx path, often through an NCPDP SCRIPT-based workflow. - Pharmacy response handling
The system records acceptance, rejection, renewal request, change request, cancellation response, fill status, or other pharmacy-originated messages. - Refill lifecycle
The patient or pharmacy initiates a refill or renewal request. The prescriber approves, denies, changes, or creates a new prescription depending on the request type and medication rules. - Medication reconciliation
Active, historical, patient-reported, dispensed, discontinued, and external medications are compared across encounters and care settings. - Discontinuation or cancellation
The clinician stops a medication or cancels a prescription. The system records the reason and sends cancellation transactions where supported and appropriate. - Audit and reporting
The system records clinically significant events, safety alerts, overrides, signing actions, transmission attempts, pharmacy responses, and controlled-substance events.
Teams that implement only the prescribing form usually find missing pieces late. Common failures include rejected pharmacy messages with no handler, duplicate refill requests, renewal messages routed to the wrong user, controlled substances signed without the required workflow, or safety alerts that clinicians override without review.

Electronic prescribing architecture: eRx, NCPDP SCRIPT, and workflow state
What NCPDP SCRIPT covers
The NCPDP SCRIPT standard supports electronic prescription transactions between prescribers, pharmacies, payers, and other entities.
Depending on the product scope, an eRx integration may need to support:
- NewRx: new prescription;
- RxRenewalRequest / RxRenewalResponse: pharmacy-originated renewal workflow;
- RxChangeRequest / RxChangeResponse: pharmacy change request workflow;
- CancelRx / CancelRxResponse: cancellation workflow;
- RxFill: fill status notification, where supported;
- Medication history transactions: medication history exchange;
- electronic prior authorization workflows: where applicable;
- long-term care workflows: if the product supports LTC prescribing.
Do not build public copy or architecture around one fixed NCPDP SCRIPT version unless that version is confirmed against the current certification program, payer requirement, network timeline, and product scope. SCRIPT version requirements can change by program and transition schedule.
Why the translation layer matters
Most EHR medication management modules should not generate NCPDP SCRIPT directly from the core clinical data model.
A safer design uses a translation layer:
- The clinician creates a medication order in the EHR.
- The module stores the order in an internal medication state model.
- Safety checks run.
- The eRx adapter converts the internal prescription state into the required NCPDP SCRIPT message.
- The outbox service transmits the message.
- The response handler updates the prescription state.
This separation matters because pharmacy transaction standards and network requirements change. If a certification program modifies a message requirement, the team should update the adapter rather than rewrite the medication lifecycle model.
The internal model should remain clinically meaningful. The adapter should handle message format, identifiers, required fields, network-specific validation, retries, and acknowledgments.
For multi-system work around EHR, pharmacy, portals, billing, and third-party APIs, see TATEEDA’s custom software integration services.
EPCS compliance: controlled-substance prescribing is a separate layer
Electronic prescribing for controlled substances, or EPCS, applies when controlled substances in DEA Schedules II through V are prescribed electronically.
EPCS is not only a login feature. It affects onboarding, identity proofing, credential management, access control, signing behavior, record retention, audit events, and application certification or audit.
The governing regulation is DEA 21 CFR Part 1311. A medication management module that supports EPCS must account for:
- prescriber identity proofing;
- two-factor authentication at signing;
- DEA registration and schedule authority;
- state authority where applicable;
- logical access controls;
- controlled-substance-specific signing screens;
- transaction integrity;
- audit events;
- application audit or certification requirements;
- recordkeeping;
- revocation of signing authority.
Two-factor authentication for EPCS
DEA Part 1311 requires the practitioner to authenticate with two approved factor types when signing an electronic controlled-substance prescription.
These factor types include:
- something the practitioner knows;
- something the practitioner has;
- something the practitioner is.
The signing event must be tied to the prescribing practitioner. The system must not allow one clinician to sign a controlled-substance prescription under another clinician’s authority.
The application must present the required prescription information for review, clearly identify the signing function, prompt for the required authentication, time-stamp the prescription, and prevent transmission of unsigned controlled-substance prescriptions.
Identity proofing and credential issuance
Before a prescriber can use EPCS signing, the system must complete identity proofing and credential issuance in a way that satisfies DEA Part 1311 and the selected credential service provider or institutional workflow.
Avoid claiming that all current implementations must follow a specific older NIST assurance level unless the project team has verified that requirement against the current DEA rule, credential provider requirements, and state rules.
Logical access control
EPCS access is not a standard user permission checkbox.
The system should record:
- who requested access;
- who approved access;
- DEA registration checked;
- schedule authority checked;
- state authority checked, where applicable;
- credential issued;
- date access became active;
- reason access was changed or revoked;
- date of revocation;
- incident record if a factor was lost, stolen, or compromised.
Access should be revoked when the prescriber leaves, loses authority, has a compromised factor, or no longer needs EPCS signing.
Build or integrate?
Building the full EPCS credentialing and signing stack internally is rarely the best first choice for a healthtech product team. The technical work is only one part. The application must also satisfy regulatory, operational, and audit requirements.
Most teams evaluate certified or audited EPCS-capable products and integrate them into the prescribing workflow. The core architecture requirement is that the signing experience remains connected to the EHR medication order, patient context, DEA-required prescription data, and audit trail.
Do not treat EPCS as a plugin added near release. It affects the medication model, prescriber onboarding, signing state, UI, audit logs, support workflows, and production readiness.
Drug database integration: why public data is not enough
The drug database layer is one of the most underestimated parts of EHR medication management development.
Public sources such as RxNorm, DailyMed, FDA drug data, and the Orange Book can support medication naming, identifiers, ingredient mapping, labeling references, and public drug information.
They do not replace a licensed clinical drug knowledge base for production safety checks.
A mature medication module often needs data for:
- drug-drug interaction checking;
- allergy and cross-sensitivity checking;
- duplicate therapy detection;
- dose range checking;
- renal dosing guidance;
- hepatic dosing guidance;
- pediatric dosing support;
- geriatric cautions;
- pregnancy and lactation risk content;
- ingredient and class mapping;
- route and dosage-form logic;
- therapeutic class grouping;
- formulary and payer-related messaging, where integrated.
Common commercial drug knowledge sources include First Databank, Wolters Kluwer Medi-Span, Lexicomp, and Oracle Health Multum. The right choice depends on licensing, content modules, API model, update process, clinical context, and the existing EHR environment.
Update pipeline requirements
Do not claim that every drug database update has a universal 24-hour legal window unless that requirement is confirmed for the specific vendor, contract, state, or regulatory context.
A safer requirement is this:
The drug database update pipeline must match the vendor’s safety-update policy, the organization’s clinical policy, and the risk profile of the prescribing system.
In practice, many systems use daily or otherwise scheduled updates, with additional procedures for urgent safety content. The engineering design should include:
- scheduled vendor-content retrieval;
- package and checksum validation;
- schema validation;
- record-count and critical-field checks;
- version comparison;
- staged loading;
- transaction-based promotion;
- rollback to the prior validated version;
- visible staleness status;
- alerting when updates fail;
- clinical review procedure for failed or delayed critical updates;
- audit history for every content release.
A partial or corrupted drug database can be more dangerous than a slightly delayed one. The system should never apply content updates silently without validation.
Drug model structure
Your internal medication model should separate at least three concepts:
| Concept | Description | Example |
|---|---|---|
| Drug product | A specific manufactured or packaged product | branded or generic product with NDC where applicable |
| Drug concept | The clinical medication concept independent of manufacturer | atorvastatin 20 mg oral tablet |
| Ingredient | The active chemical entity | atorvastatin calcium |
Most clinical decision support rules operate at ingredient, class, dose, route, or therapeutic group level rather than only at product level.
For example, a clinician may choose a specific product in the UI, but DDI logic needs the active ingredient. Duplicate therapy logic may need a therapeutic class. Dose-range logic may need route, form, patient weight, renal function, age, and current lab context.
RxNorm concept unique identifiers, or RxCUIs, can help normalize medication concepts, but the mapping still requires governance. Your system needs to know where RxNorm ends and where commercial CDS content begins.

Drug-drug interaction checks and allergy checks are not the same system
One common architecture mistake is building one generic “safety check” service for all medication alerts.
Drug-drug interaction checks and drug-allergy checks have different logic.
Drug-drug interaction checks
DDI checks compare a new medication against the patient’s active medication list. They may evaluate:
- ingredients;
- dose;
- route;
- duration;
- metabolic pathway;
- therapeutic class;
- administration timing;
- severity;
- patient-specific factors;
- monitoring recommendations.
Example: a new medication may increase bleeding risk when combined with an anticoagulant. The alert may depend on drug pair, dose, patient age, renal function, active diagnoses, and monitoring plan.
Drug-allergy checks
Drug-allergy checks compare the proposed medication against the patient’s allergy and intolerance list.
They must account for:
- exact ingredient match;
- drug class;
- cross-sensitivity;
- reaction type;
- reaction severity;
- allergy vs. intolerance;
- date recorded;
- source of allergy information;
- whether the patient later tolerated a related drug;
- certainty of the allergy entry.
A patient with nausea listed as a “codeine allergy” should not always trigger the same workflow as a patient with anaphylaxis to an opioid. The system needs a data model that distinguishes allergy, intolerance, adverse reaction, severity, certainty, and clinical relevance.
Why is one generic safety service risky
If DDI and allergy logic share the same path too tightly, changes become dangerous.
Examples:
- lowering DDI severity thresholds accidentally changes allergy behavior;
- an allergy update is missed because it is not modeled as an interaction;
- override reasons are reused across unrelated alert types;
- pharmacy informatics cannot tune alert classes independently;
- audit reports cannot separate allergy overrides from interaction overrides.
A safer design uses separate rule domains that feed a common alert presentation and audit framework.
Clinical decision support alert architecture
A medication management module should assign each CDS alert a severity tier and workflow behavior.
| Severity tier | Workflow behavior | Typical meaning |
| Absolute stop | The action cannot proceed under configured policy | Prohibited order, missing legal requirement, or unresolvable safety issue |
| Restricted override | The clinician can proceed only with required rationale, permissions, or an alternative workflow | High-risk medication decision requiring documented judgment |
| Interruptive soft stop | The clinician must review and acknowledge before continuing | Significant risk or monitoring concern |
| Advisory | Displayed without blocking workflow | Low-level guidance, monitoring note, or informational warning |
The clinical drug database may provide severity levels, but the organization still needs a pharmacy informatics review. A hospital ICU, oncology clinic, pediatric clinic, and primary-care practice may not use the same alert policy.
Alert fatigue is not a UI inconvenience. It is a patient safety risk. If clinicians receive too many low-value alerts, they learn to move through them quickly. The alerts that matter become easier to miss.
What to monitor after go-live
Medication CDS requires operational monitoring, not only launch testing.
Track:
- alert frequency by type;
- override rate by alert;
- override rate by clinician role;
- overrides missing rationale;
- alerts fired after the order was already signed;
- alerts suppressed by configuration;
- duplicate alerts in one session;
- high-severity alerts overridden repeatedly;
- alerts that never change clinician behavior;
- reported safety events linked to medication ordering.
A pharmacy informatics team should review this data regularly and tune alert behavior with clinical leadership.
Hypothetical failure pattern
Imagine a new EHR deployment where the safety engine technically works. Every rule fires as configured. The problem is volume.
During morning rounds, a clinician sees dozens of advisory medication alerts. Most involve low-level interactions or medications the patient has already tolerated for years. After repeated low-value warnings, the clinician begins moving through the alerts quickly.
A high-risk allergy or interaction warning appears in the same session. It looks like every other alert. The clinician overrides it.
In that scenario, the root problem is not necessarily a code defect. The alert system may be firing exactly as configured. The failure is missing clinical governance: no severity tuning, no alert-volume review, no first-week override-rate analysis, and no process for suppressing low-value alerts without losing high-risk signals.
Medication safety logic must be clinically reviewed before launch and monitored after launch.
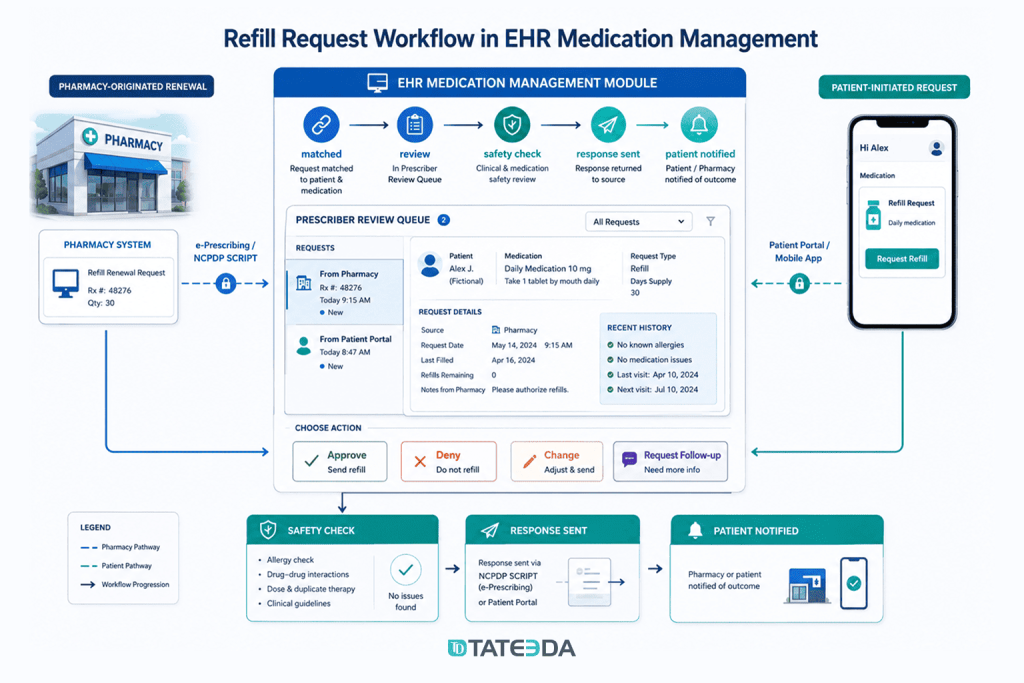
Refill request workflow architecture
Refill requests come through more than one path. Treating all refill requests as the same event creates duplicate orders, lost pharmacy messages, and unsafe approvals.
Pharmacy-originated renewal requests
A pharmacy-originated renewal request usually arrives through an eRx network transaction such as an NCPDP SCRIPT renewal request.
The pharmacy sends this when the patient requests a continuation, and the original prescription has no refills left or requires prescriber authorization.
The system must:
- parse and validate the message;
- match it to an existing prescription or medication history item;
- identify the original prescriber or covering pool;
- route it to the correct workflow queue;
- show pharmacy, medication, patient, and original prescription context;
- check whether the medication is eligible for renewal;
- run safety checks again before approval;
- return the appropriate renewal response;
- record the request and response in the patient record.
The response may be approval, denial, replacement with a changed prescription, or another supported response type depending on the transaction and workflow.
Do not publish a universal response-time requirement unless it is confirmed against the current network policy, payer program, client policy, and state rules. The safer engineering requirement is that every renewal request has a due time, status, owner, escalation path, and transmission audit.
Patient-initiated refill requests
Patient-initiated refill requests usually come through a patient portal or mobile application.
They are different from pharmacy-originated renewal messages.
The request should be tied to:
- patient identity;
- active medication list item;
- last prescription;
- last dispense information if available;
- preferred pharmacy;
- remaining quantity if known;
- last appointment;
- required labs or monitoring;
- controlled-substance eligibility;
- refill policy;
- prescriber or care-team owner.
A portal request may result in a new prescription, a renewal, a denial, a request for appointment, a request for labs, or routing to a care-team queue.
The patient-facing UX should avoid promising that a refill is approved before clinician review, payer review, pharmacy processing, and controlled-substance rules are resolved.
For patient-facing refill, access, payment, and communication interfaces, see TATEEDA’s patient portal development services.
Controlled substance refill rules
Schedule II controlled substances cannot be refilled under federal rules. Each dispense requires a new prescription, though federal rules allow certain multiple-prescription workflows under specific conditions.
Schedules III and IV have federal refill limits. State law, payer policy, organizational policy, and specialty-specific practice may be more restrictive.
The important engineering principle is this: Do not hard-code one universal refill policy.
The system should parameterize refill rules by:
- DEA schedule;
- state;
- medication;
- prescriber authority;
- patient age;
- diagnosis or treatment plan where appropriate;
- days’ supply;
- quantity;
- number of prior refills;
- date of original prescription;
- last fill date;
- earliest fill date;
- pharmacy response;
- PDMP policy where applicable.
A controlled-substance refill should fail at the workflow eligibility stage before a clinician signs an order that cannot be transmitted or filled.
Patient safety rules beyond DDI and allergy checks
A mature medication management module should support more than drug-drug interactions and allergy alerts.
Duplicate therapy alerts
Duplicate therapy logic catches cases where two drugs in the same class or therapeutic category are active at the same time.
Example: The patient is already taking one beta-blocker, and the clinician adds another. This may not be a classic drug-drug interaction, but it can still be a prescribing error.
The rule needs:
- active medication list;
- therapeutic class mapping;
- start and stop dates;
- medication status;
- patient-reported vs. prescribed distinction;
- tapering or transition logic;
- override rationale when clinically intended.
Dose range checking
Dose checking may require:
- age;
- weight;
- body surface area;
- renal function;
- hepatic function;
- route;
- indication;
- frequency;
- maximum daily dose;
- pediatric dosing rules;
- geriatric cautions;
- recent lab data.
Pediatric dosing is especially sensitive because many medications depend on mg/kg logic. The system must know whether the patient weight is current enough for dosing use.
Renal and hepatic dose adjustment
Renal dosing rules require current kidney-function data. The system may need to calculate or consume creatinine clearance, eGFR, or another approved measure, depending on the organization’s policy and drug database content.
Do not assume the newest lab is always valid for dosing.
The rule may need:
- lab timestamp;
- specimen validity;
- inpatient vs. outpatient context;
- recent dialysis status;
- acute kidney injury flags;
- patient age and weight;
- drug-specific renal threshold.
Hepatic dosing is often harder because structured hepatic function indicators may be incomplete or scattered across labs, diagnosis lists, and notes.
Pregnancy and lactation alerts
The old FDA pregnancy letter categories should not be the core data model for new medication safety logic.
The FDA’s Pregnancy and Lactation Labeling Rule removed the A, B, C, D, and X categories from prescription drug labeling and replaced them with more detailed content for pregnancy, lactation, and reproductive potential.
Modern pregnancy and lactation safety logic should use drug database content aligned with current labeling, plus structured clinical context where available.
The system may need:
- pregnancy status;
- estimated gestational age;
- lactation status;
- medication risk information;
- indication;
- urgency;
- alternative medication availability;
- clinician rationale;
- patient counseling documentation where required.
This requires data governance because pregnancy status may appear in multiple places: problem list, encounter diagnosis, obstetric history, lab results, notes, or patient intake.
Formulary and prior authorization alerts
Formulary and prior authorization logic is not the same as clinical drug safety logic, but it has clinical consequences.
If a patient cannot fill a medication due to coverage issues, therapy may be delayed or abandoned. This is especially important for oncology, specialty medications, chronic disease management, and expensive therapies.
A medication module may need:
- formulary status;
- preferred alternatives;
- step therapy requirements;
- prior authorization requirement;
- payer-specific benefit data;
- estimated patient cost;
- pharmacy availability;
- electronic prior authorization initiation;
- appeal or substitution workflow.
This content typically comes from payer, pharmacy benefit, or ePA integrations, not from the clinical drug database alone.
For teams connecting prescribing with reimbursement, claims, balances, and payer workflows, TATEEDA also provides medical billing software development.
Hypothetical implementation lesson
Imagine a specialty EHR team that launches with strong DDI and allergy checking but postpones formulary and prior authorization integration.
The prescribing workflow works clinically. The problem appears later at the pharmacy. Patients arrive and discover that therapy requires prior authorization or a payer-preferred alternative. Staff begin calling payers manually. Clinicians lose time. Patients experience delays.
The missing feature is not just administrative. In some specialties, access friction can delay treatment.
For high-cost or specialty medication workflows, formulary and prior authorization visibility should be planned early, even if full automation is released later.
HIPAA, DEA, Surescripts, and state compliance: what affects the architecture
A medication management module sits across several compliance domains.
HIPAA
Medication data is protected health information when it is linked to an identifiable patient.
The HHS HIPAA Security Rule establishes standards for protecting electronic protected health information through administrative, physical, and technical safeguards.
HIPAA Security Rule planning should cover:
- access control;
- user identity management;
- emergency access;
- audit controls;
- integrity controls;
- transmission security;
- risk analysis;
- risk management;
- business associate agreements;
- incident response;
- role-based access;
- offboarding;
- vendor access;
- backups and disaster recovery.
Avoid publishing rigid statements such as “HIPAA requires AES-256 at rest and TLS 1.2 or higher in transit” unless the statement is framed as a common implementation choice rather than a universal HIPAA mandate.
A better architecture statement is:
The system should use modern encryption in transit and at rest, strong key management, secrets control, access logging, and risk-based safeguards that satisfy HIPAA Security Rule requirements, organizational policy, and applicable contracts.
Audit logging and retention
Do not state that all audit logs must automatically be retained for six years.
HIPAA includes six-year retention requirements for required documentation, but not every operational log automatically has the same retention period. DEA EPCS rules include their own recordkeeping expectations. State rules, payer contracts, malpractice policies, and organizational policies may require different retention periods.
Medication management systems should separate:
- HIPAA security audit events;
- EPCS signing and controlled-substance events;
- clinical CDS alert events;
- override rationale records;
- eRx transmission logs;
- pharmacy response logs;
- medication history changes;
- user access logs;
- data-change logs;
- support and administrative logs.
Each category needs a retention policy approved by legal, compliance, clinical leadership, and security.
DEA EPCS
EPCS architecture must address:
- identity proofing;
- two-factor signing;
- DEA registration and schedule authority;
- logical access control;
- controlled-substance signing screen;
- required electronic signing behavior;
- application audit or certification;
- incident detection;
- recordkeeping;
- revocation of access;
- pharmacy transmission requirements.
Surescripts and network policies
Network certification may involve:
- enrollment;
- prescriber identity verification;
- pharmacy directory behavior;
- message conformance;
- transaction testing;
- workflow review;
- error-rate monitoring;
- production approval;
- version and message-scope confirmation.
Do not assume that development completion equals production approval.
State pharmacy and PDMP requirements
State requirements may affect:
- eRx mandates;
- controlled-substance prescribing;
- PDMP query requirements;
- refill rules;
- day-supply limits;
- opioid prescribing workflows;
- benzodiazepine workflows;
- pharmacy transfer rules;
- prescribing exceptions;
- delegate access.
The medication module should keep state-specific rules configurable rather than buried in application code.
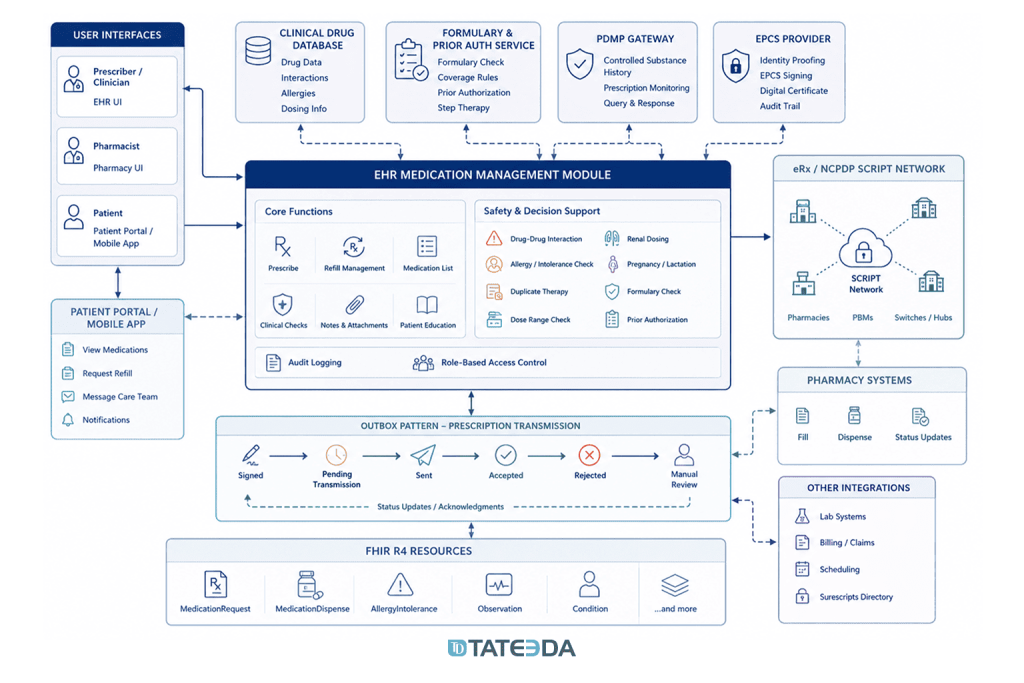
Integration architecture: how the system fits together
A production-grade EHR medication management module may need integrations with:
- eRx network;
- EPCS identity and authentication provider;
- clinical drug database;
- formulary and benefit source;
- electronic prior authorization service;
- PDMP or PDMP gateway;
- pharmacy directory;
- EHR patient demographics;
- problem list;
- allergy list;
- active medication list;
- medication history;
- labs;
- vitals;
- pregnancy status where available;
- height and weight;
- billing and claim systems where relevant;
- patient portal.
Each external dependency has its own format, authentication model, latency, downtime pattern, and error behavior.
Use an outbox pattern for prescription transmission
A clinician should not lose a signed prescription because an external network call fails at the wrong moment.
A safer architecture uses an outbox pattern:
- The prescriber completes the order.
- Safety checks run.
- The prescriber signs.
- The system writes the signed prescription and required state to local storage.
- The system creates a pending transmission record in an outbox.
- A separate worker transmits the message.
- Responses update prescription state.
- Failures are retried, escalated, or routed for manual review.
- Clinicians see clear transmission status.
This avoids coupling the user interface directly to network availability.
A network outage should not erase the clinician’s work. Depending on policy and prescription type, the system may allow local drafting, signing, queuing, or delayed transmission while clearly showing that the prescription has not reached the pharmacy.
Model medication state explicitly
Medication state should be explicit, not inferred from scattered fields.
Possible states include:
- draft;
- ready for review;
- safety check pending;
- safety check failed;
- signed;
- pending transmission;
- transmitted;
- accepted;
- rejected;
- change requested;
- cancellation requested;
- cancelled;
- renewal requested;
- renewal approved;
- renewal denied;
- dispensed, where fill data is available;
- discontinued;
- entered in error.
Each state transition should capture:
- actor;
- timestamp;
- source;
- reason;
- related external message;
- patient;
- medication;
- prescription identifier;
- prior state;
- new state.
This makes pharmacy failures, audit events, refill workflows, and patient-support tickets easier to resolve.
FHIR R4 mapping: useful, but not a replacement for eRx transactions
FHIR R4 can represent medication concepts and support downstream data exchange.
Useful resources include:
- MedicationRequest: medication order or prescription request;
- MedicationDispense: supply of medication, often in response to a prescription;
- MedicationStatement: record of medication use or patient-reported medication;
- MedicationAdministration: administered medication;
- Medication: medication concept;
- AllergyIntolerance: allergy and intolerance data;
- Observation: labs, vitals, pregnancy-related observations, renal function context where appropriate;
- Condition: diagnoses and problem list items that may support medication decisions.
For EHR and care coordination workflows, mapping internal medication state to FHIR can help patient portals, payer tools, analytics systems, care-management systems, and external apps access medication data consistently.
But FHIR should not be described as replacing NCPDP SCRIPT for prescription routing to pharmacies. In U.S. eRx, NCPDP SCRIPT remains central to pharmacy transaction workflows.
The practical design is usually both:
- internal and downstream clinical data represented with FHIR-friendly models;
- pharmacy transaction exchange handled through NCPDP SCRIPT and network-specific certification.
TATEEDA experience relevant to medication and pharmacy workflows
TATEEDA’s healthcare and pharmaceutical software materials describe several adjacent capabilities that matter for EHR medication management architecture:
- prescription and claims workflow automation;
- patient access portals;
- pharmacist and pharmacologist workspaces;
- customer claim management;
- eRx management tooling;
- bulk document processing with OCR;
- pharmacy claim processing and medication fulfillment;
- healthcare payment portals;
- business automation for pharmaceutical operations.
These are not the same as claiming that every EHR medication module described in this article already exists as a public TATEEDA case. The stronger and safer point is this:
Medication management systems reuse many patterns from pharmacy-adjacent healthcare builds: state management, third-party API integration, PHI-aware access, queue handling, document ingestion, alerting, patient-facing workflows, and audit-conscious architecture.
SCRx pharmacy claims and medication fulfillment
TATEEDA’s SCRx pharmacy claims automation case involved pharmacy claim processing and medication fulfillment workflows, including backend development, cloud integration, third-party API integration, automated bulk PDF import, OCR, and system alerts.
That case is relevant to medication management architecture because prescription-related systems often need the same engineering patterns:
- durable workflow states;
- queue-based processing;
- document and message ingestion;
- exception handling;
- user-facing alerts;
- integration monitoring;
- operational visibility.
Patient payment and access workflows
TATEEDA’s custom patient payment portal case is not a prescribing system, but it is relevant to secure patient-facing healthcare workflows. Medication refill requests, refill-status notifications, medication cost estimates, and payment-related workflows often require similar controls: authenticated access, role-based permissions, transaction history, patient-facing UX, and secure data exchange.
Pharmaceutical business automation
The pharmaceutical business automation case is relevant for prescription-adjacent operations where order processing, data handling, shipping workflows, and partner processes need structured software support.
For a new medication module, TATEEDA can help review the architecture around prescribing, refill handling, safety checks, pharmacy messaging, controlled-substance workflows, and clinical record integration.
For broader planning, see healthcare software development and software cost estimation.
FAQ: EHR medication management development
What does it cost to license a clinical drug database?
Pricing depends on vendor, modules, deployment model, patient or encounter volume, content scope, support model, and contract terms.
Do not publish a fixed price range unless it comes from a current quote. A project budget should account for licensing, implementation, update pipelines, clinical validation, testing, and ongoing content governance.
Ask vendors specifically about:
- DDI content;
- allergy content;
- dose checking;
- renal and hepatic dosing;
- pregnancy and lactation content;
- pediatric support;
- RxNorm mapping;
- formulary modules;
- API vs. file-based delivery;
- update cadence;
- BAA requirements;
- audit and support terms.
How long does Surescripts or eRx network certification take?
Certification timelines vary. Plan for weeks to months rather than a short engineering sprint.
The timeline depends on:
- message scope;
- product maturity;
- test environment readiness;
- prescribing workflow complexity;
- team responsiveness;
- required corrections;
- partner engineering availability;
- controlled-substance scope;
- production approval steps.
Start the network certification workstream early. Do not wait until the prescribing UI is finished.
Can we use open-source NCPDP libraries?
Possibly, but with caution.
The library must support the required NCPDP SCRIPT version and message types for your certification scope. It must also be maintainable when the standard, network requirements, or certification tests change.
Even with a library, your team still owns:
- message validation;
- field mapping;
- test coverage;
- error handling;
- certification fixes;
- logging;
- retry logic;
- security review;
- ongoing maintenance.
Do we need EPCS on day one?
If your product will support electronic prescribing of controlled substances, plan EPCS from the start.
If your product will not support controlled substances at all, EPCS may not be required for the initial scope. But this must be validated against client requirements, state rules, market expectations, and prescribing workflows.
Do not assume EPCS applies only to Schedule II drugs. Electronic prescribing of controlled substances across DEA Schedules II through V requires controlled-substance-specific compliance.
Adding EPCS later can be disruptive because it affects prescriber onboarding, identity proofing, access control, signing workflow, audit records, and production certification.
What should override logging include?
For high-risk medication alerts, the override log should capture:
- patient identifier;
- prescriber identity;
- encounter or order context;
- medication;
- alert type;
- severity;
- rule version;
- drug database version;
- exact alert text or alert identifier;
- override action;
- prescriber rationale;
- timestamp;
- resulting prescription;
- whether the prescription was transmitted.
This log should be queryable by pharmacy informatics, clinical safety, compliance, and product support teams according to role-based access rules.
Should hard-stop alerts ever be overridable?
Sometimes yes, sometimes no. It depends on clinical policy, alert type, legal requirement, and risk.
A missing EPCS signing requirement should not be overridable by ordinary clinical judgment. A high-risk drug interaction may require a restricted override if the prescriber documents rationale and monitoring.
The system should distinguish:
- legal or technical blockers;
- absolute clinical stops;
- restricted clinical overrides;
- soft stops;
- advisories.
Do not put all interruptive alerts into one category.
Can FHIR MedicationRequest be the system of record for prescribing?
FHIR MedicationRequest is useful for representing medication orders and exchanging medication order data. Whether it should be the internal source of truth depends on the product architecture.
Many teams use an internal medication state model and map to FHIR resources for interoperability. That can be safer than trying to force all prescribing workflow state into external FHIR resource fields.
The important rule is that your internal state model must preserve the data needed for clinical workflow, pharmacy transactions, auditing, safety rules, and downstream exchange.
Can an EHR medication management module support patient refill requests?
Yes, but portal-based refill requests should be treated as a separate workflow from pharmacy-originated renewal requests.
A portal request should show the patient’s active medication, preferred pharmacy, last fill information where available, monitoring requirements, refill eligibility, and status. It should not promise approval before clinician review, controlled-substance checks, payer requirements, and pharmacy processing are complete.
Building this right: where engineering and clinical safety intersect
A medication management module is a patient-safety system.
The highest-risk mistakes are rarely cosmetic. They usually appear in state transitions, missing rules, stale drug data, unreviewed alert behavior, poor refill routing, weak controlled-substance access controls, or incomplete audit history.
The engineering principles that matter most:
- Separate clinical domains clearly
Do not collapse DDI, allergy, duplicate therapy, dosing, formulary, and EPCS logic into one generic service. - Version drug knowledge and CDS configuration
When someone asks what DDI severity rule was active on a specific date, the system must answer. - Build an outbox for network transmission
External pharmacy networks can fail. The prescribing workflow must show status clearly and recover safely. - Treat EPCS as architecture, not authentication polish
Controlled-substance signing affects identity proofing, access, signing, audit, and support workflows. - Make refill paths explicit
Pharmacy-originated renewal requests and patient-initiated portal requests are different workflows. - Monitor alert behavior after launch
Override rates, alert volume, and alert usefulness should be reviewed with clinical informatics. - Display drug database staleness
If content updates fail, clinical users and operations teams need visibility. - Test with pharmacists and clinicians, not only QA engineers
QA can test software behavior. Clinical reviewers catch medication-risk scenarios that normal test plans miss. - Check FDA CDS scope by intended use
The FDA Clinical Decision Support Software guidance explains how CDS software functions are assessed. Some CDS functions may be excluded from the device definition, while others may still be device software. Intended user, transparency, data type, and ability to independently review the recommendation basis matter. - Document failure handling before go-live
What happens if the eRx network is unavailable, the drug database update fails, the EPCS provider is down, PDMP is unavailable, or the pharmacy sends a rejection? Each failure needs an owner and workflow.
TATEEDA’s healthcare software architects can help review the integration architecture, safety-rule model, refill workflows, audit design, and EPCS readiness of an EHR medication management module before development begins.
Medication systems do not need theatrical claims. They need careful architecture, clinical review, up-to-date drug knowledge, controlled-release processes, and failure paths that protect patients when dependencies fail.
To discuss your EHR medication management module, contact TATEEDA or request a software cost estimate.






