AI in Healthcare Staffing: How US HR Teams Use AI to Fill Roles Faster

Slava Khristich

Vlad Nazarov

What you’ll learn from this article:
- Where AI in healthcare staffing fits in the pipeline (source → screen → schedule → verify → onboard)
- Which workflows get the fastest ROI (and which are risky)
- How generative AI in HR is used without turning hiring into a black box
- The custom AI software development compliance guardrails: HIPAA, bias risk, and auditability.
On paper, hiring a nurse or a medical biller looks like “post job → interview → offer.”
In real life, AI in healthcare staffing exists because the funnel is clogged: chronic shortages trigger overtime and burnout, candidates drop off when the process drags, and HR teams get stuck in credentialing loops (licenses, background checks, references, onboarding documents).
Meanwhile, demand for nurses and other medical professionals keeps rising. The Association of American Medical Colleges projects the U.S. could face a physician shortage of up to 86,000 by 2036 (AAMC projections), and the American Association of Colleges of Nursing continues to warn that the RN pipeline cannot expand fast enough to meet demand (AACN nursing shortage fact sheet).
This article is a practical guide to AI in healthcare staffing shortage realities: what AI actually does in recruiting and staffing, what AI tools do healthcare HR teams use, and where HIPAA + legal/technical limits “bite” (especially when candidate data overlaps with employee health info, immunizations, drug screens, or occupational health records).
We’ll also show examples of AI used in healthcare staffing software development, including an AI voice agent for medical staffing solutions that can call candidates and run structured screening interviews (Incredible Health’s Gale and Lyn).
Why is TATEEDA qualified to talk about AI-enhanced HR systems?
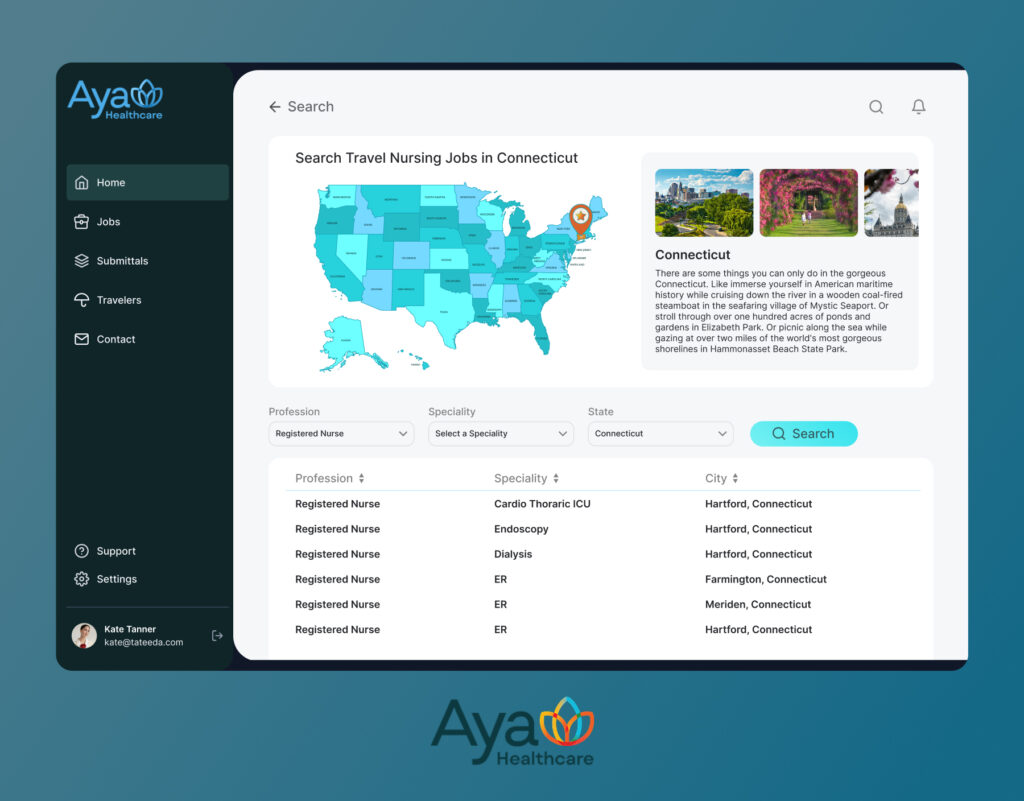
TATEEDA is a San Diego provider of healthcare software development services. Our portfolio includes a long-term partnership with one of the largest healthtech travel nurse staffing agencies, AYA Healthcare. We’ve helped their team architect, build, test, and deploy several mission-critical infrastructure applications used by travel nurses, healthcare representatives, and administrators. This work has included AI-supported components for workforce calculations, qualification scoring, candidate-to-role matching, and document/credentialing workflows.

BeOnBoard (Byoxon): Small Business Management Solution
We’ve also built an internal product we use ourselves for team and client management: BeOnBoard, a web-based small business suite that brings timesheets, team rates, billable hours, CRM, and P&L tracking into one workspace, alongside other day-to-day operations features.
We originally created it to reduce tool-switching and keep delivery, finance, and account teams working from the same source of truth when managing projects and clients. More recently, we expanded BeOnBoard with a full CRM (including deployable contact forms) and added AI-assisted capabilities such as candidate skill scoring to support faster, more consistent screening and decision-making.
This product can be considered as…
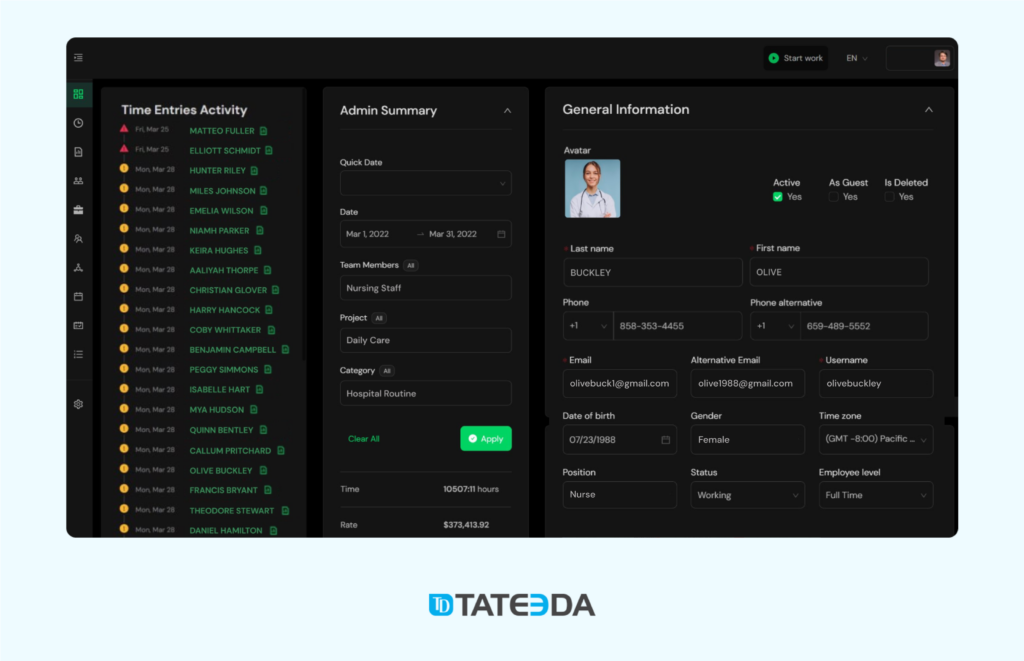
Table of Contents
Market situation, trends, and facts in the US healthcare context
Staffing shortage reality: who’s hit hardest
In the U.S., healthcare hiring pressure isn’t limited to clinicians. The most impacted groups typically include:
- Registered nurses (RN), LPNs, CNAs, and allied health (rad techs, lab, respiratory therapy)
- Behavioral health (counselors, therapists)
- Revenue cycle roles (coding, billing, prior auth)
- Patient access/call center and scheduling teams
The challenge isn’t just “not enough applicants.” It’s the friction—process steps that cause delays and drop-offs.
Healthcare hiring funnel friction points (why it’s uniquely hard)
Healthcare HR has to manage constraints that most industries don’t:
- License verification and primary-source checks
- Background checks, drug screening, and required documentation
- Credentialing and onboarding checklists that differ by role/facility
- Shift coverage volatility (urgent needs spike suddenly)
- High churn in certain roles, creating constant backfill
- Multi-site staffing (same role, different facility rules and schedules)
Macro trend #1: HR is moving from experiments to implementation
Across HR, adoption is accelerating. A Gartner survey found 38% of HR leaders were piloting, planning, or already implementing GenAI as of early 2024. In healthcare, the urgency is sharper because vacancy days translate into lost capacity and staff burnout.
Macro trend #2: from “ATS-only” to workflow automation
Traditional ATS workflows often stop at “track applicants.” Modern AI HR software focuses on moving candidates through the funnel:
- screening + matching
- engagement + reminders
- scheduling
- credentialing handoffs
- onboarding workflow completion
Macro trend #3: conversational AI and voice agents are getting real
Chatbots moved first (SMS + web chat), and now voice is catching up. Paradox openly claims it can “automate 90% of the hiring process” with two-way messaging and automated scheduling. Meanwhile, healthcare-specific players are building voice agents that conduct structured interviews at scale (again: Gale and Lyn).
Macro trend #4: skills-based hiring (especially for clinical roles)
Healthcare is increasingly formalizing competency frameworks (specialty experience, certifications, shift readiness, unit fit) and using AI to rank candidates on skills + constraints, not just keywords.
Snapshot table: why the pressure is structural (not a temporary blip)
| Signal | What it means for hiring | Source |
|---|---|---|
| Physician shortage up to 86,000 by 2036 | More competition for clinical talent; faster hiring cycles win | AAMC projections |
| RN shortage expected to intensify | Larger reliance on pipeline + retention + faster screening | AACN fact sheet |
| 38% of HR leaders piloting/implementing GenAI (2024) | AI becomes “normal” tooling in HR operations | Gartner press release |

Where AI Fits in the Staffing Workflow & Practical Use Cases
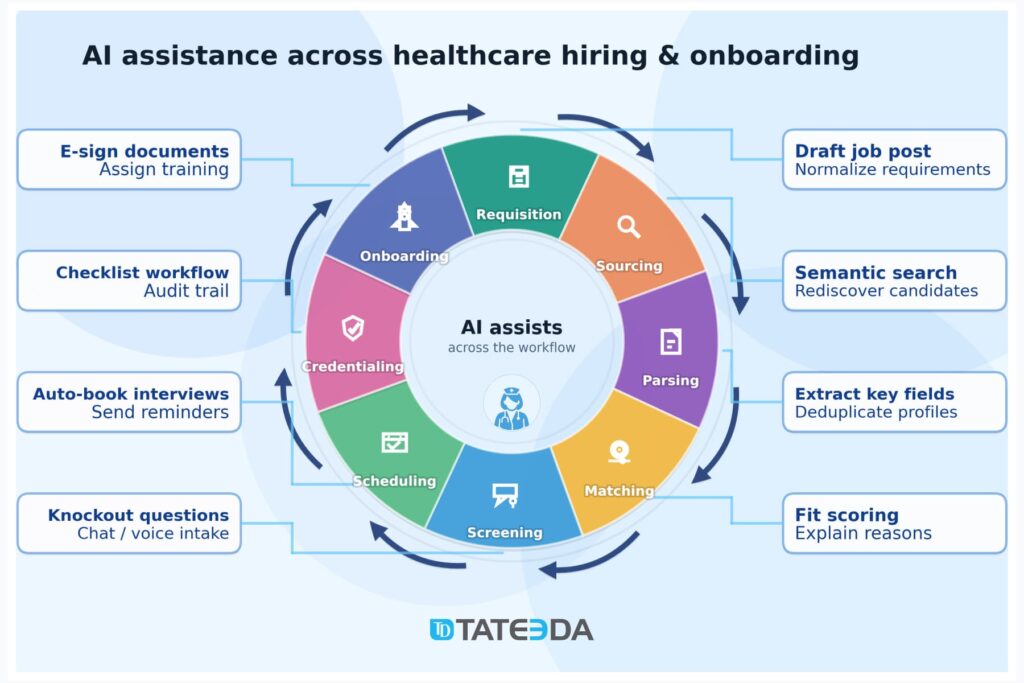
Think of AI and HR as a pipeline optimizer. Here’s where AI agents for HR typically fit, step by step:
- Sourcing & rediscovery:
Search inside your ATS/CRM to “rediscover” silver-medalist candidates, then expand outward (job boards, marketplaces). This is one of the easiest wins for AI in healthcare staffing because the data already exists—HR can’t manually re-check thousands of profiles every week. - Resume intake & parsing:
AI parses resumes into structured data, deduplicates profiles, and aligns them to job requirements. This is the backbone of modern AI HR systems. - Skill matching & scoring:
This is where how to use AI in HR becomes concrete: you combine hard constraints (license, certification, location, shift type) with soft signals (specialty experience, tenure, unit background) to generate an explainable match score. - Pre-screening & Q&A (chat or voice):
High-volume roles benefit from structured screening questions (knockout criteria, availability, shift preferences). Here you’ll see examples of AI used in healthcare staffing, like conversational bots that respond instantly, keep candidates warm, and reduce drop-off. - Scheduling automation:
This is often the “silent killer” of time-to-hire: back-and-forth emails and missed calls. Tools like Paradox focus heavily on automating this layer. - Credentialing support:
AI can manage document collection and checklist completion; however, healthcare needs strong governance here—errors are costly. If any step touches PHI (occupational health, immunizations, etc.), you’ll need HIPAA-grade controls and often a Business Associate Agreement (BAA) posture. - Offer & onboarding:
Auto-generate offer packets, policy acknowledgements, training assignments, and reminders—without turning the process into spam. - Workforce ops layer (optional extension):
Some orgs extend AI beyond hiring into float pool optimization and internal shift marketplaces—useful when hiring can’t keep up with demand.
HIPAA note (keep it simple): if a vendor is acting as a “business associate” and handling PHI, HR teams need to treat that as a compliance boundary, not just an IT checkbox (HHS guidance on business associates).
Technologies and Features behind AI HR Solutions
When people say AI in healthcare staffing, they often picture a single “smart tool” that magically finds nurses. In practice, modern AI HR software is a stack of building blocks—each doing one job well—wired together into a workflow that HR teams can actually trust.
Think of it like a hospital: you don’t just have “healthcare,” you have triage, labs, imaging, pharmacy, and charting that all connect. HR AI works the same way.
1) LLMs and NLP: the “language engine”
This layer powers generative AI in HR tasks where the input and output are mostly text.
Typical uses include:
- Drafting job descriptions from a short role brief (then keeping tone and compliance consistent)
- Generating candidate summaries (“Why this person matches the ICU RN role”)
- Producing outreach messages that don’t sound like spam
- Answering recruiter questions (“What’s our shift differential policy?”) via internal knowledge search
The key is guardrails: a good system shows sources, flags uncertainty, and avoids inventing facts (especially around pay, benefits, or credential requirements).
2) Matching models: from “keyword search” to skill-based fit
Candidate matching usually blends two approaches:
- Semantic matching (embeddings + vector search):
Resumes and job descriptions are converted into numeric “meaning vectors.” This helps identify strong matches even when the wording differs (e.g., “telemetry” vs. “cardiac monitoring”). - Rules + weighted scoring (hard constraints):
Healthcare hiring has non-negotiables: active license, specific certification, location radius, shift type, and unit experience. Rules enforce the must-haves; scoring ranks the nice-to-haves.
This is where AI agents for HR become useful: they can run the matching workflow repeatedly, adjust weights, and surface “explainable” shortlists for recruiter review.
3) Conversation layer: chat and voice that moves candidates forward
If your funnel leaks candidates, the conversation layer patches it. A well-built AI voice agent for medical staffing solutions usually includes:
- ASR (speech-to-text) to understand candidates on calls
- TTS (text-to-speech) to speak naturally back
- Dialog orchestration to keep the interview structured (and compliant)
- Call routing + human handoff when a case is complex or sensitive
- ATS/CRM logging so conversations become trackable hiring data, not “random calls.”
The goal isn’t to replace recruiters—it’s to remove phone-tag and run consistent pre-screens at scale.
4) Data layer: integrations, auditability, and retention controls
AI cannot fix broken data. Most value comes from connecting:
- ATS/HRIS records (applications, stages, offers)
- Credentialing systems (licenses, renewals, verifications)
- Background check providers (status, results, disputes)
Add governance on top: audit logs, retention rules, and “why this candidate was ranked” artifacts.
5) Integration patterns: how everything connects
Common integration mechanisms:
- APIs + webhooks for real-time updates (stage changes, interview scheduled)
- ETL to a data warehouse for reporting and forecasting
- RPA for legacy portals where APIs don’t exist
6) Security and compliance architecture: HIPAA-first reality
Even HR workflows can touch sensitive health-related data (occupational health, immunizations, drug screens). A HIPAA-aware approach typically includes:
- Encryption in transit/at rest, strong access controls, least privilege
- PHI segmentation + redaction before text is sent to models
- Clear BAA expectations (or strict “no PHI allowed” boundaries)
- Model governance: prompt logging, evaluations, red-teaming, and bias testing.
| Building block | What it does in staffing | What “good” looks like |
|---|---|---|
| LLM/NLP | Summaries, outreach, Q&A, drafting | Sources, guardrails, no hallucinations |
| Matching | Finds + ranks candidates | Explainable scores + hard constraint rules |
| Voice/chat | Screening + scheduling | Human handoff + ATS logging |
| Data layer | Connects systems of record | Audit logs + retention controls |
| Integrations | Moves data end-to-end | APIs/webhooks first; RPA as fallback |
| Security/compliance | Protects sensitive data | HIPAA boundaries, redaction, least privilege |

Legal + Tech Limitations: the Red Lines of AI HR in Healthcare
If you’re adopting AI in healthcare staffing, assume you’re automating decisions and communications about people in a regulated environment. That means your risks come from three directions at once: privacy/security, employment law, and “AI reliability.” Good AI HR software doesn’t just “rank candidates”—it defines guardrails so automation can’t quietly become a liability.
HIPAA: where it does and doesn’t apply
In plain terms: employment records are generally not PHI under HIPAA, even if they contain health-related details. However, healthcare organizations often touch data that can be PHI depending on where it lives and how it’s used—for example:
- Occupational health clinic records are maintained like medical records
- Drug screening results coming from a covered provider workflow
- Immunization documentation stored in clinical systems
- Health plan/benefits data managed under covered-entity operations
So the practical red line is this: treat anything that might include medical-status details as “PHI-risk,” even if HR assumes it’s “just hiring data.” That drives your architecture choices.
BAA vs “no PHI allowed”: you must pick one
A surprising number of AI vendors won’t sign a Business Associate Agreement. If that’s the case, your safe options are:
- Hard “no PHI allowed” boundary (data minimization + policy + technical controls), or
- Choose a vendor/workflow that supports HIPAA obligations (and can contractually commit to them)
“Policy-only” doesn’t work. You need enforcement: input validation, file controls, and ideally DLP-style checks.
Employment law and fairness: AI can’t be the gatekeeper
AI-driven hiring still falls under anti-discrimination rules. The safest operational model for how to use AI in HR is:
- AI can recommend, summarize, and prioritize
- Humans must approve rejections or “final shortlist” steps
- Decisions should carry reason codes (license mismatch, shift constraints, missing certification)—not opaque scores
This improves defensibility, candidate experience, and internal trust.
Technical limits that show up in real hiring ops
These issues are common even in strong implementations:
- Hallucinations: incorrect candidate summaries or invented claims
- Data quality: duplicates, stale licenses, inconsistent job titles, missing fields
- Integration drift: ATS says one thing; scheduler/calendar says another
- Model drift: ranking subtly changes over time as data and models evolve
- Explainability gaps: you can’t justify outcomes if the model is a black box
Practical red-line checklist
- No PHI in tools without an appropriate contractual/security posture
- No fully automated rejection without human review
- No scoring without explainability artifacts and audit logs
- No AI-generated promises about pay/benefits/role requirements unless template-controlled
| Risk area | What can go wrong | Control that actually works |
|---|---|---|
| PHI spillover | accidental PHI enters AI | data minimization + enforced input rules + segregation |
| Bias/adverse impact | unfair screening outcomes | human-in-the-loop + outcome monitoring + reason codes |
| Hallucinations | misinformation to candidates/managers | constrained templates + verification rules + QA sampling |
| Data drift | silent degradation | monitoring KPIs + periodic revalidation |
Vendor Landscape in the U.S. + Quick Comparison Table
When someone asks what AI tools healthcare HR teams use, the honest answer is: they use a stack, not one product. In a typical AI in healthcare staffing setup, AI shows up as features layered into an ATS/CRM for resume parsing and candidate matching, screening tools (chat or voice) to reduce drop-off, scheduling automation to cut no-shows, and credentialing/onboarding workflows to keep licenses and documents moving.
In other words, AI and HR in healthcare usually means stitching together a few AI HR software components so the hiring funnel runs faster and more consistently, especially during an AI in healthcare staffing shortage.
Bucket 1: ATS/HCM platforms with AI features (system of record)
These platforms store requisitions, applicants, stages, offers, and reporting. Their AI commonly covers:
- Resume parsing and structured candidate profiles
- Skills extraction and basic matching
- Workflow automation (routing, reminders, approvals)
- Analytics (funnel conversion, time-to-fill)
Reality check: feature depth varies by product tier and configuration. For healthcare, the question isn’t “do they have AI?”—it’s “can the AI operate within your privacy and audit requirements?”
Bucket 2: Sourcing + matching layers (find talent faster)
These tools sit above the ATS and focus on discovery/rediscovery:
- Semantic search across resumes and profiles
- Filters for credentials, specialty experience, location, shift constraints
- Talent pool “remining” (silver medalists, past applicants)
Best for: teams that feel they’re losing candidates simply because they can’t find them fast enough.
Bucket 3: Healthcare-first marketplaces/staffing platforms
Healthcare-native platforms often focus on specific roles (e.g., nursing) and try to shorten time-to-hire via:
- Better matching tuned to clinical roles
- Structured screening flows
- Faster candidate engagement
Best for: high-volume clinical hiring where speed and candidate experience drive outcomes.
Bucket 4: Conversation + scheduling automation (reduce drop-off)
This category is where chat/voice tools shine:
- Screening Q&A (knockout questions)
- Scheduling and rescheduling automation
- Reminders and follow-ups
- Recruiter handoff when needed
If you’re evaluating an AI voice agent for medical staffing solutions, validate the basics: consent scripts, call logging policies, escalation paths, and what data is stored where.
| Layer you’re buying | Common vendor examples | What it solves | What to validate (non-negotiables) |
|---|---|---|---|
| ATS/HCM AI | Workday, UKG, iCIMS, (mid-market: Greenhouse, Lever) | Structured hiring workflow + reporting + automation inside the system of record | Audit logs; role-based access; explainability artifacts; integration depth (ATS↔calendar↔HRIS); data retention controls |
| Matching / talent intelligence | Eightfold AI, SeekOut | Faster shortlist + talent rediscovery (past applicants, silver medalists) + skill-based ranking | Hard-constraint support (license/cert/shift/location); bias monitoring on outcomes; reason codes (why ranked/rejected); model change control |
| Chat / voice automation | Paradox | Lower candidate drop-off + screening Q&A + scheduling/rescheduling + reminders | Consent/recording policy; human handoff; data minimization; ATS write-back; logging of conversations + auditability |
| Healthcare marketplace / role-specific platforms | Incredible Health (nursing-focused) | Faster access to clinical talent pools + structured engagement for specific roles | Data ownership/retention; integration with ATS; credentialing workflow fit; boundaries on sensitive info (PHI-risk) |
Build vs Buy: Custom AI for Healthcare HR
In AI in healthcare staffing, “buy vs build” usually comes down to how many exceptions your workflow has. If your hiring pipeline is fairly standard—post a role, screen, schedule, and onboard—then buying an AI HR software layer on top of an ATS can be enough to relieve AI in healthcare staffing shortage pressure without rebuilding your operating model.
In that “buy” scenario, AI is mostly accelerating the same steps you already do: sorting applicants faster, finding past candidates you forgot you had, nudging people to show up, and keeping the funnel moving. It’s often the right choice when your team is primarily asking “what AI tools do healthcare HR teams use?” and wants quick wins with a predictable setup.
Custom work becomes justified when healthcare-specific friction is the problem you need to solve. Credentialing logic is a classic trigger: multi-state licenses, expiring certifications, unit-specific requirements, and verification workflows that don’t map neatly to generic rules. The second trigger is multi-facility complexity—float pools, travel radius, shift volatility, redeployment across sites, and internal mobility.
That’s where AI agents for HR start to make sense: not just recommending candidates, but coordinating work across systems while staying inside policy (collect documents, reconcile checklists, propose matches, schedule interviews, and route edge cases to humans).
A quick “buy is enough” vs “custom is justified” lens:
- Buy is enough when roles are standard, the pipeline is simple, PHI exposure is low, and your ATS/HRIS stack is mature.
- Custom is justified when credentialing logic is complex, scheduling is multi-site and volatile, you need an internal talent marketplace, you have a unique scoring rubric, or you need a stronger compliance posture and auditability model than vendors typically provide.
Here’s the decision trade-off in one view:
| Factor | Buy (vendor) | Build (custom) |
|---|---|---|
| Speed | Faster to launch | Slower start, faster iteration later |
| Control | Limited configuration | Full control over rules + UX |
| Compliance posture | Depends on the vendor | Designed around your risk model |
| Integration depth | Standard connectors | Deep, workflow-native integrations |
| TCO | Lower upfront, ongoing seats | Higher upfront, lower marginal cost at scale |
| Vendor lock-in | Often higher | Lower if you own workflow + data |
| Auditability | “As provided” | Tailored logs + explainability |
Estimated Cost and Duration of AI-enhanced HR System Development
When people ask how to use AI in HR for healthcare, they often assume the “AI part” is the hard part. In practice, timelines and budgets are driven by integrations, data readiness, and governance—especially if you’re adding an AI voice agent for medical staffing solutions.
Tier A is the lightweight path: AI add-ons and workflow automation inside your existing stack. Think parsing and dedupe, candidate rediscovery, basic screening questions, scheduling nudges, and simple reporting. This typically lands in 2–6 weeks and often sits around $15k–$60k, depending on how messy ATS data is and how many workflows need standardization.
Tier B is where AI in healthcare staffing becomes interactive: a chat/voice layer that does structured intake, asks knockout questions, proposes times, and syncs updates back to your ATS—plus basic scoring (certifications + experience + availability) with human review. That’s usually 6–12 weeks and $60k–$180k, plus ongoing usage costs (voice minutes, model calls).
Tier C is full custom orchestration: matching + workflow routing + credentialing support + onboarding automation + analytics, with strong audit trails and role-based access. In effect, you’re building a staffing operating layer with AI and HR capabilities embedded. That tends to be 3–6+ months and $180k–$600k+, depending on integration breadth and compliance controls.
What pushes cost/time up (or down):
- Integrations: ATS, HRIS, scheduling, credentialing, background checks, communications.
- Data cleanup: duplicates, inconsistent job titles, missing credential fields, legacy notes.
- Security/compliance: logging, encryption, retention policies, access reviews, audit-ready trails.
- Human-in-the-loop design: review queues, escalation rules, overrides, approvals.
- Evaluation/QA: false match rates, consistency of screening, reliability of scheduling flows.
- Usage volumes: voice minutes and LLM tokens, plus peak hiring season traffic.
Final word
Healthcare hiring is no longer “post and wait.” In AI in healthcare staffing, the winners are the teams that treat recruiting like an operational workflow: faster outreach, fewer no-shows, clearer qualification decisions, and smoother credentialing and onboarding. Across the article, we walked through what US healthcare HR teams actually do with AI today, why the market is moving toward stacks (not single tools), and where technical limits and HIPAA expectations shape what’s realistic.
This is also where TATEEDA can help. We build AI-enhanced HR systems for healthcare organizations that want practical outcomes, not demos. That can mean adding safe automation to an existing ATS, or designing AI agents for HR that coordinate tasks across sourcing, screening, scheduling, credentialing, and onboarding, with human approvals where it matters.
Typical ways we support healthcare HR and staffing teams:
- Design the workflow and scoring logic (skills, certifications, availability, facility rules).
- Build an AI voice agent for medical staffing solutions for structured intake and scheduling, with tight guardrails.
- Integrate ATS/HRIS/scheduling/credentialing tools and clean up the data flow.
- Put HIPAA-minded controls in place: data minimization, access rules, logging, and audit-friendly decision trails.
If you’re deciding whether to buy, build, or combine both, we can map your current pipeline, pinpoint the bottlenecks, and propose a build plan that fits your systems, timelines, and compliance posture.





